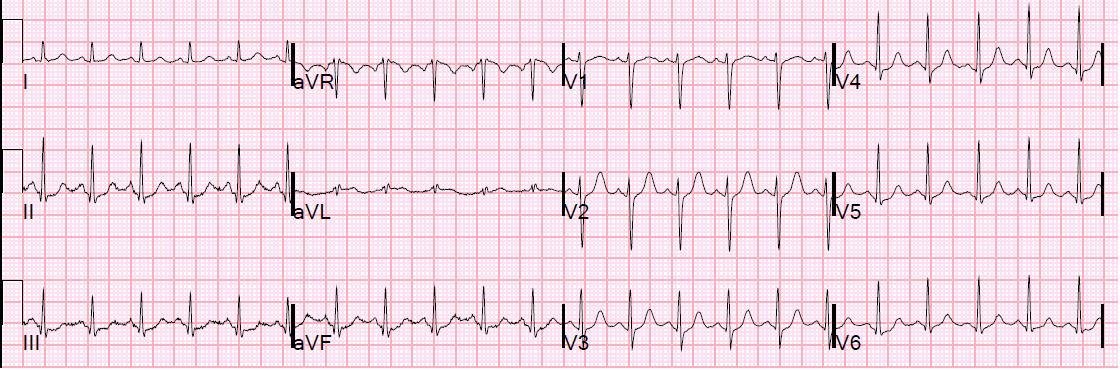
A middle-aged male presented pain free after an episode of chest pain. Here is the initial ECG (sorry some is cut off — it is an iPhone shot from a friend):
 |
| There is LBBB with appropriate discordance of all ST segments. Anterior ST elevation is appropriate, with highest ST/S ratio of 3.5/28 = 0.125 (mean normal = 0.11; normal up to 0.19). There are concordant T-waves in V5 and V6. This is a nonspecific sign of NonSTEMI. |
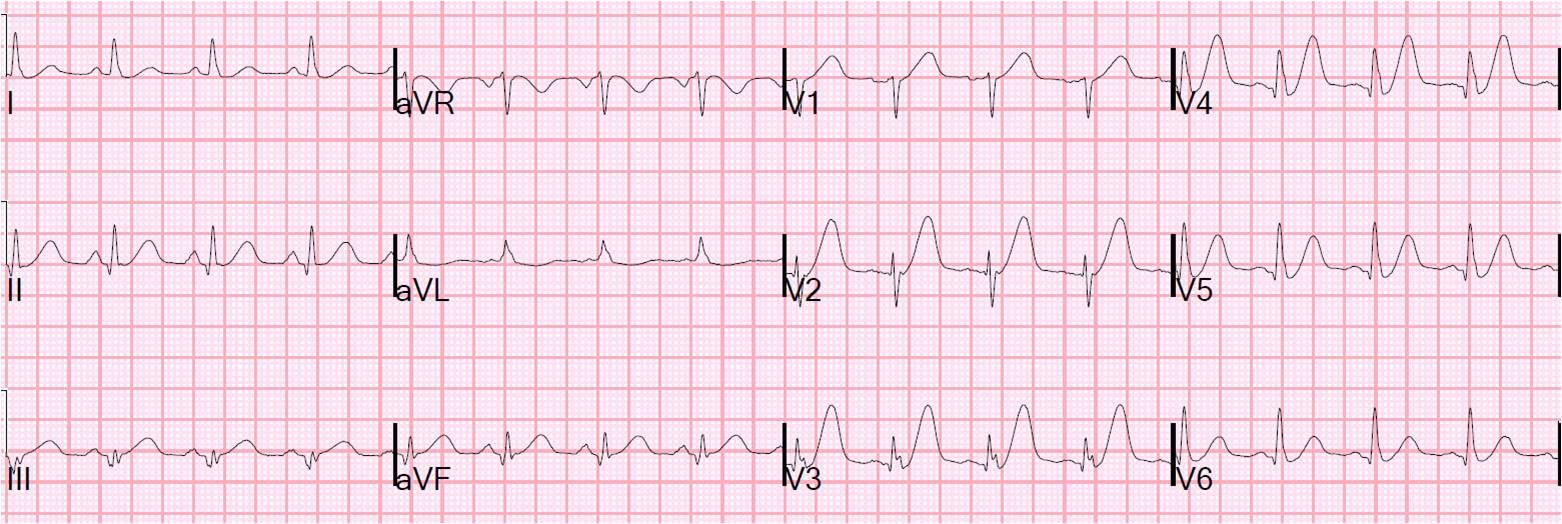
5 minutes later, the patient had crushing chest pain, and this ECG was recorded (again, some of limb leads are cut off):
 |
| Now there is concordant ST depression in V2 and V3. This is a relative change of approximately 5 mm(!). There is excessively discordant ST depression in V4-V6. (V4 ratio is 2/6 = 0.33; V5 ratio = 2.5/6.5 = 0.38; V6 = 2/6.5 = 0.31). Thus, there is ischemic ST depression in V2-V6. In normal conduction, ST depression from V2-V6 is often due to subendocardial ischemia, whereas when limited to V1-V4, it is usually posterior STEMI. Either way, this is a patient with acute coronary syndrome with chest pain. If you cannot control the symptoms with medical therapy, then the patient must go to the cath lab. |
I have written about excessively discordant ST elevation, but have not mentioned excessively discordant ST depression. In our study of LBBB with and without coronary occlusion, just one lead with excessively discordant ST depression or ST elevation, as defined as a ratio of ST depression (or elevation) to the preceding R-wave (or S-wave), greater than 0.25, was very specific for ischemia (in our study, for occlusion). More recent analysis of the data showed that 0.20 was probably a better cutoff.
The physician called the interventionalist, who did not agree there was ischemia on the ECG. The patient was started on nitroglycerine IV and the pain subsided, as did the ECG findings.
The patient was admitted pain free on nitro and no immediate cath was done. The troponin I peaked later at 0.18 ng/ml.
The next AM, the patient had another episode of pain that could not be resolved with maximal medical therapy. He went for emergent cath, which showed a proximal lad 95% stenosis with deep ulcer and a 90% mid lad stenosis. Both were stented.
Later, the troponin peaked at 5.6, and echo showed anteroseptal hypokinesis with EF <40%.
So this was LBBB with concordant and excessively discordant ST depression, representing ST depression in leads V2-V6, completely consistent with subendocardial ischemia due to profound LAD ischemia.