A 54 year old male suddenly collapsed. He had not complained of symptoms prior to this. He received bystander CPR, then was defibrillated when the medics arrived. He arrived in the ED awake. The following ECG was recorded:
 |
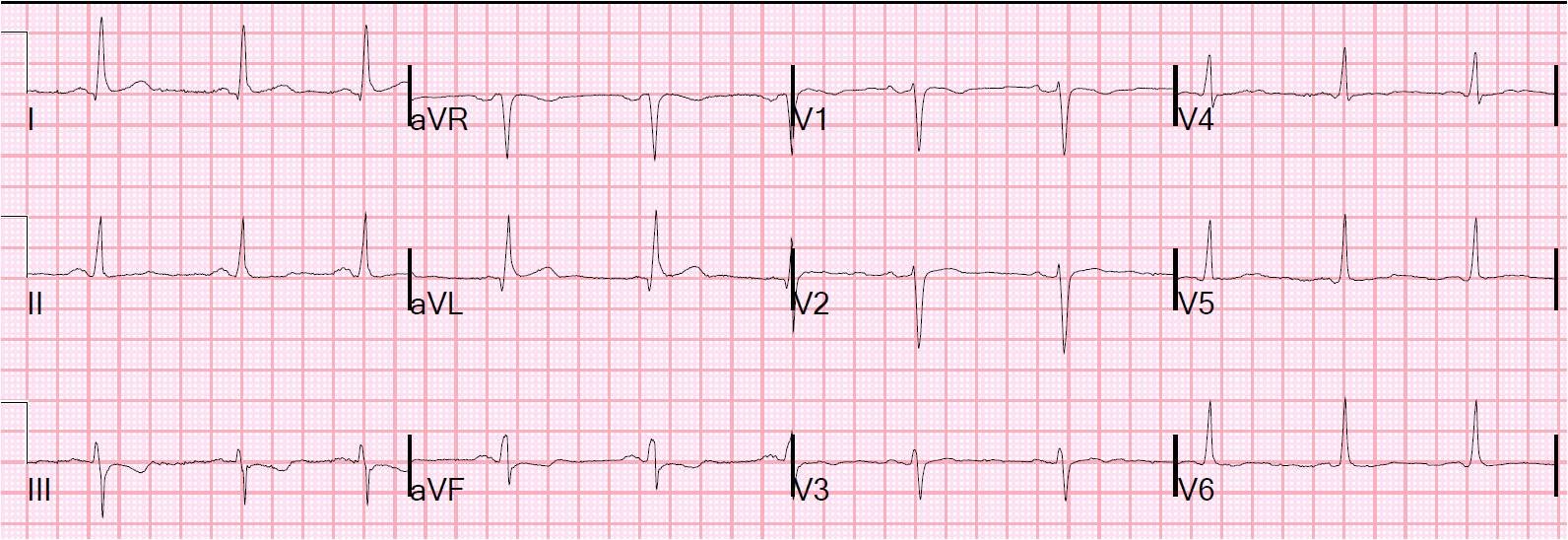
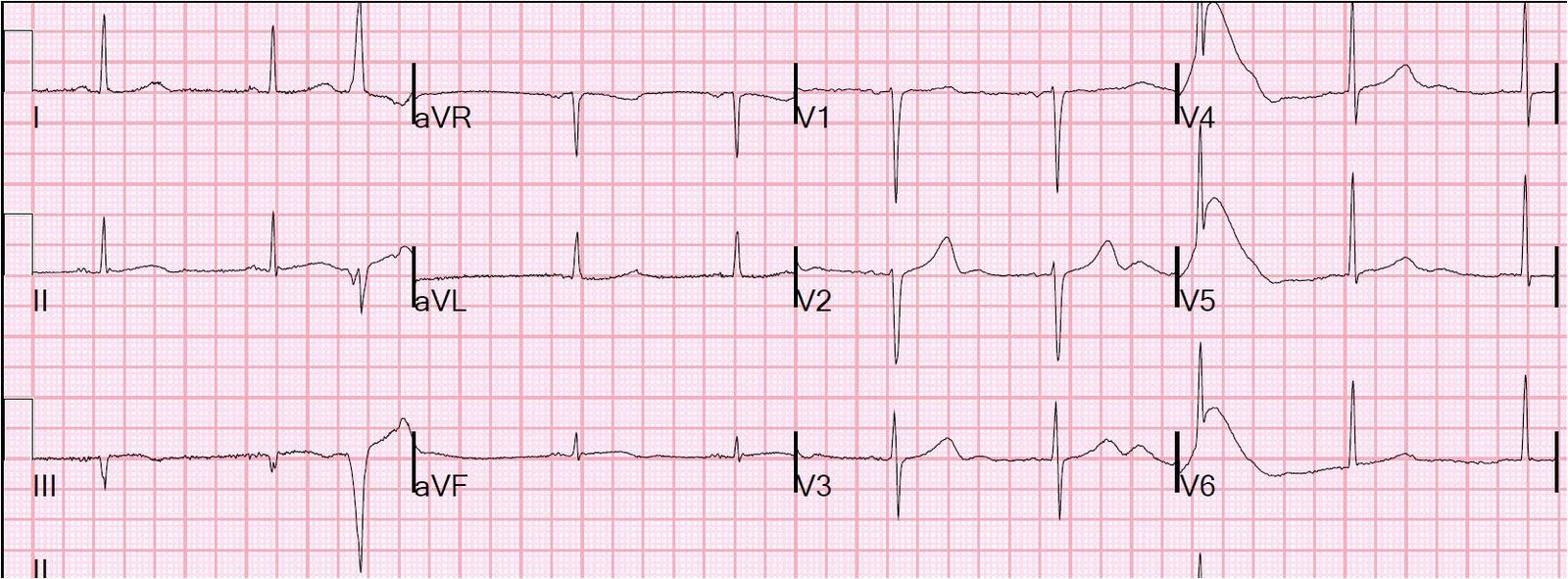
| There is sinus tachycardia with diffuse ST depression (I, III, III, aVF, V2-V6), with obligatory ST elevation in aVR (ST depression maximal in leads II and V4 establishes the ST vector as upward and rightward; there must be ST elevation in aVR). |
This is typical of NonSTEMI with ischemia from acute 3-vessel ischemia or left main stenosis. It establishes ongoing ischemia, though sometimes may be residual after cardiac arrest. So a repeat ECG should be done a short time later in order to establish whether there is, indeed, ongoing ischemia. Thrombolytics are never given for such an ECG, but angiogram and PCI are indicated if medical therapy alone does not control the ischemia.
Amiodarone 150 mg was given, along with aspirin, heparin, and eptifibatide. Because of tachycardia and thus a risk for cardiogenic shock, no beta blocker was given. BP was adequate and so nitroglycerine drip was started. Clopidogrel (or any thienopyridine) was not used because the ST elevation in aVR makes the probability of CABG high.
15 minutes later, the patient was awake enough to take a history. He stated that he had ongoing chest pressure, strongly suggesting ongoing ischemia. The leads were placed for a repeat 12-lead ECG, and we were talking to the patient when the ECG tech said, “Hey, guys, uh……” We looked up and this is what we saw:
 |
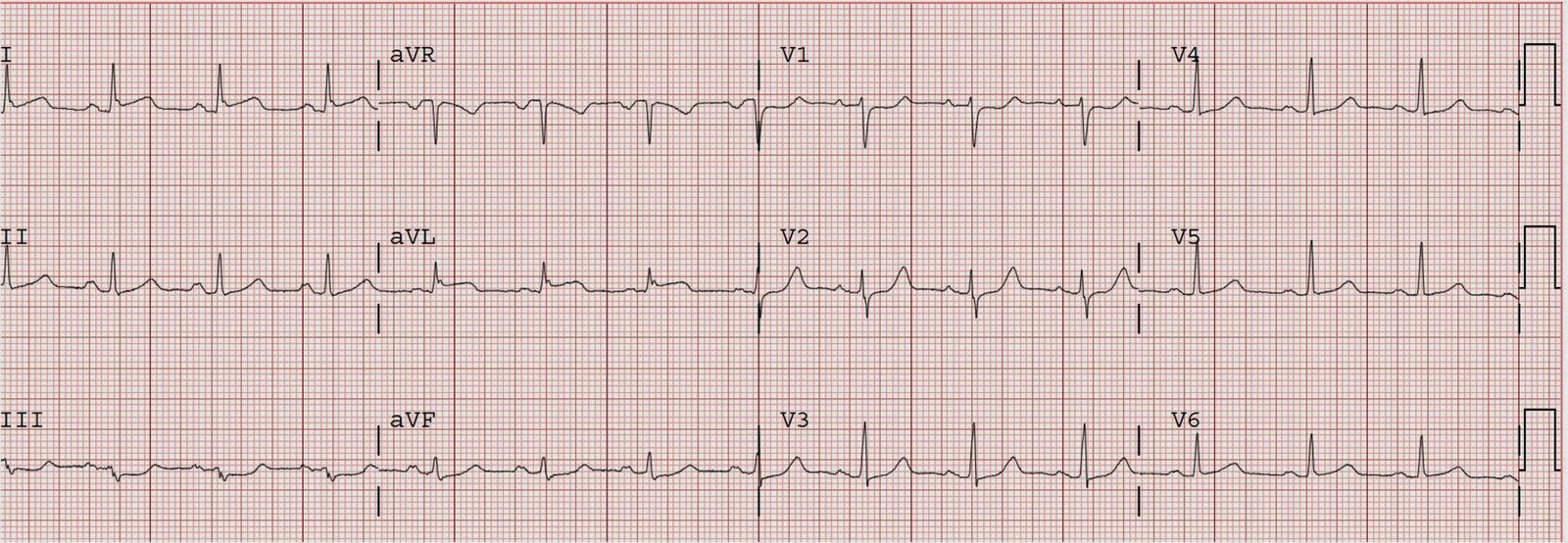
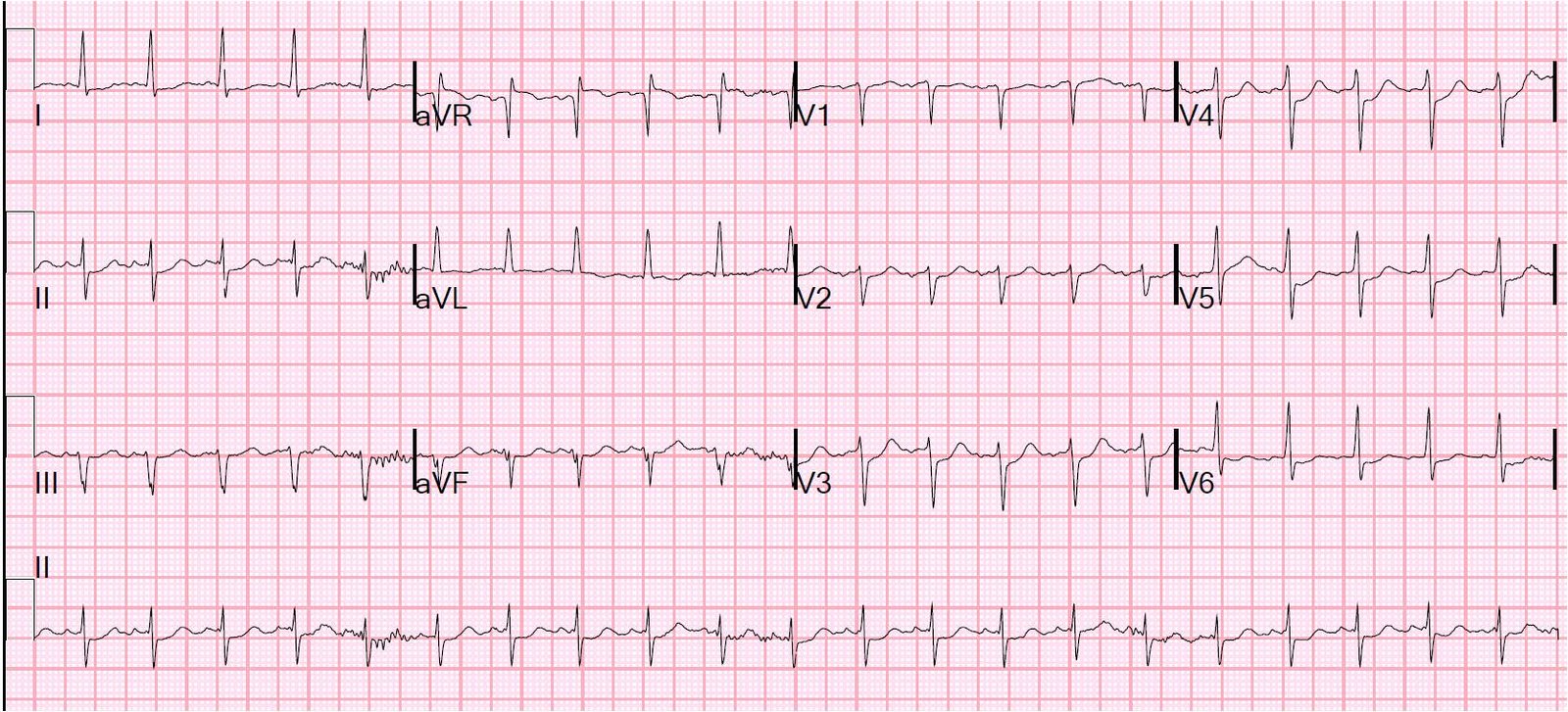
| 12-lead ventricular fibrillation. Not seen very often!! Notice how similar ventricular fibrillation is to torsade. By the way, the computer read: sinus tachycardia with frequent multiform PVCs!!!! |
The patient was awake but becoming obtunded when he was defibrillated successfully with one shock; he did not remember it.
Recurrent v fib in the setting of ischemia is diagnostic of ongoing and uncontrolled ischemia. The only way to control this is with PCI, if angiogram shows a lesion amenable to therapy.
A second 150 mg dose of amiodarone was given.
Angiogram showed 3-vessel disease and 3 lesions in the LAD which were stented. He did well.