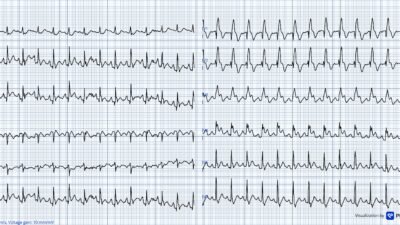
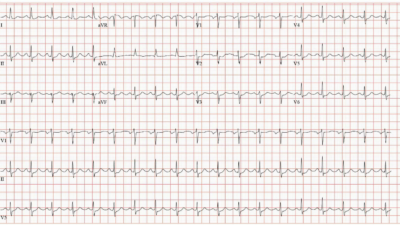
An 80 year old male with h/o CABG presented with CP. Here is his initial ECG (which was identical to his prehospital ECG) at 1517:
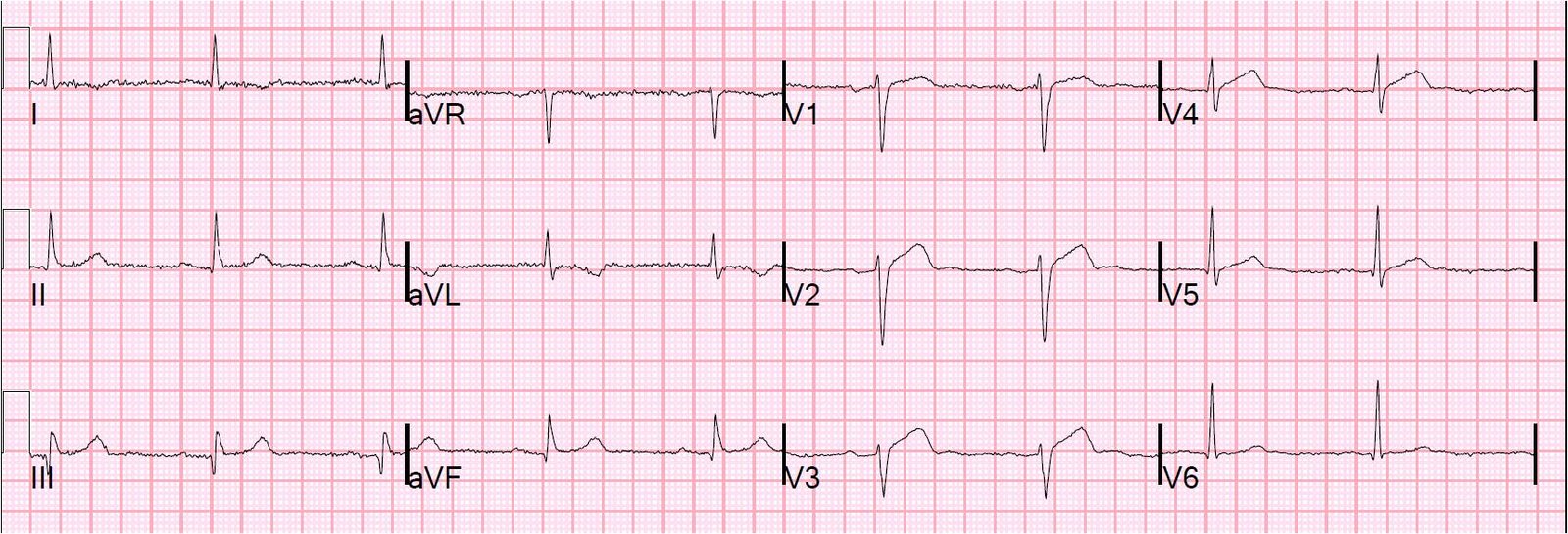 |
| There is evidence old inferior MI. What is the acute finding? Answer below. |
This is another acute LAD occlusion. There is slightly more than 1 mm of ST elevation in V2 and V3 at the J-point. Is this normal or is it pathologic (STEMI or even LVH)? First, it is clearly not LVH. Second, normal variant ST elevation always has good R-wave progression. If you add up the R-wave amplitudes in V2-V4 and it is less than 15 mm (here it is 11 mm), it is almost never early repolarization. Finally, using the equation (see sidebar excel spreadsheet) and the computerized QTc of 399 ms, the value is 24.4 which is greater than 23.4 and heavily favors STEMI.
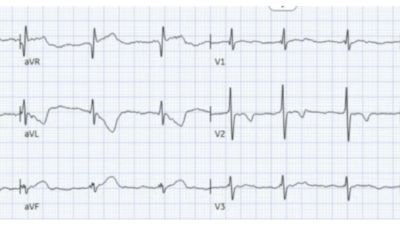
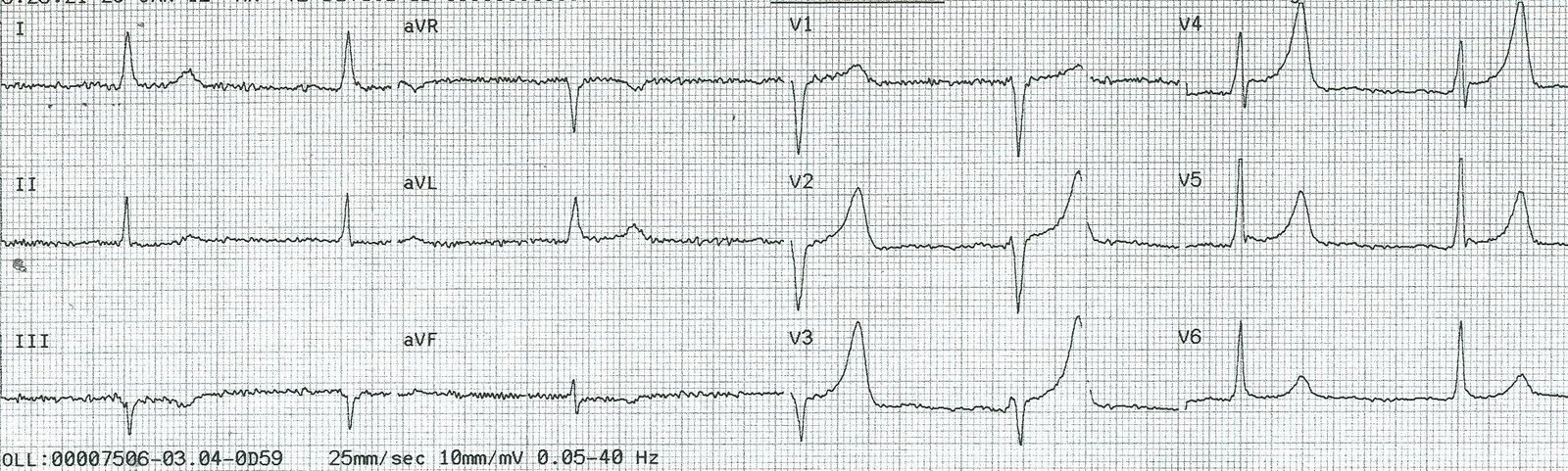
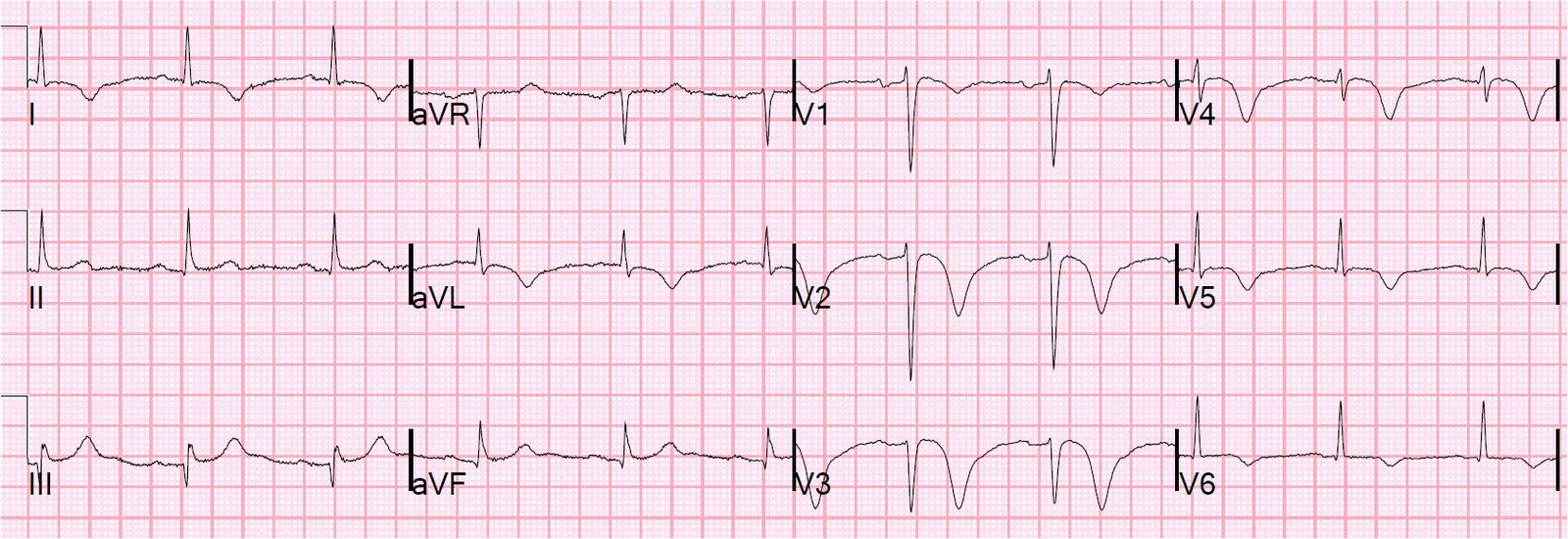
The resident saw this but the faculty was not convinced. Chest pain continued and this repeat ECG was recorded at 1652:
 |
| There is slightly more ST elevation |
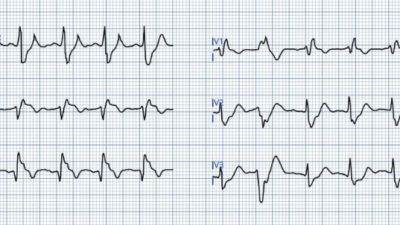
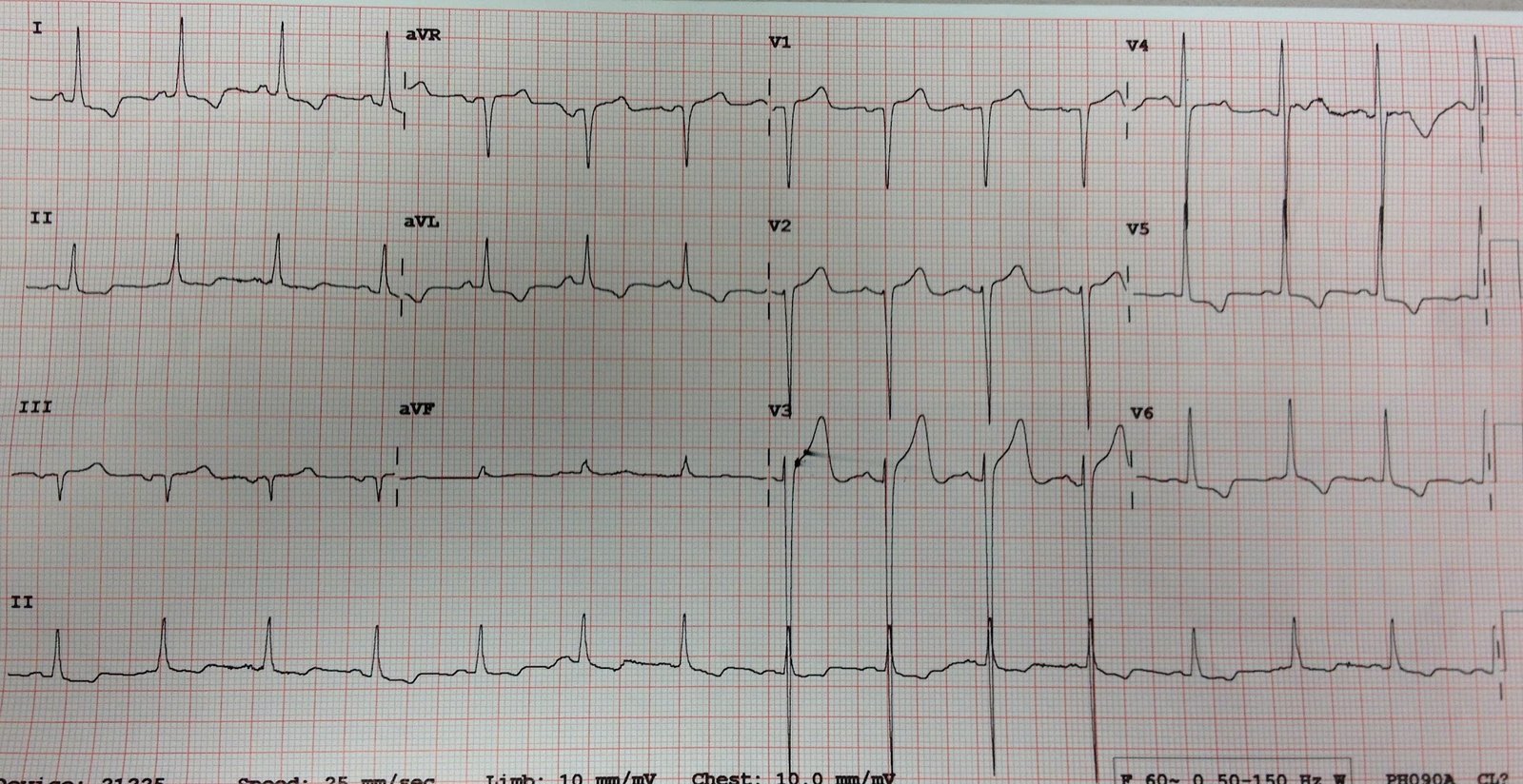
A 3rd ECG was recorded at 1720:
 |
| There is still more ST elevation and the T-waves are larger. |
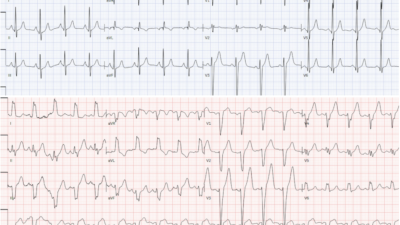
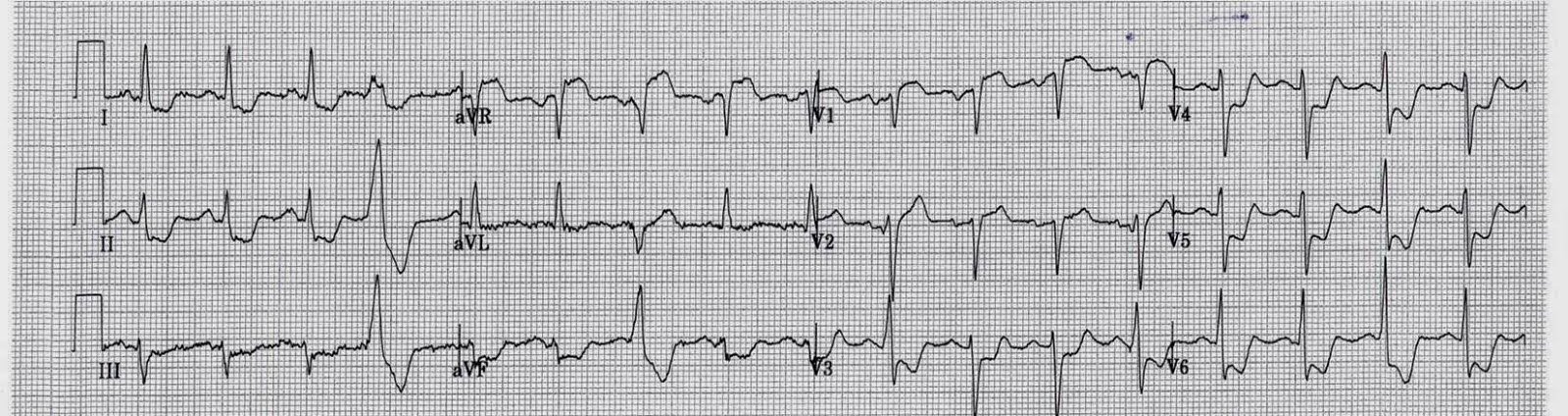
At this point, the cath lab was activated. Angiogram revealed an acutely occluded saphenous vein graft to the LAD which was opened with PCI. Here is the post cath ECG:
 |
| Now there are T-wave inversion analogous to Wellens’ syndrome. These are reperfusion T-waves, also seen in I and aVL, indicating involvement of the lateral wall from a proximal LAD. |
The next day ECG is here:
 |
| T-wave inversion is evolving as it normally does after reperfusion. |
Troponin I peaked at 38 ng/ml. Notice how important serial ECGs are if the initial ECG is nondiagnostic or not recognized.