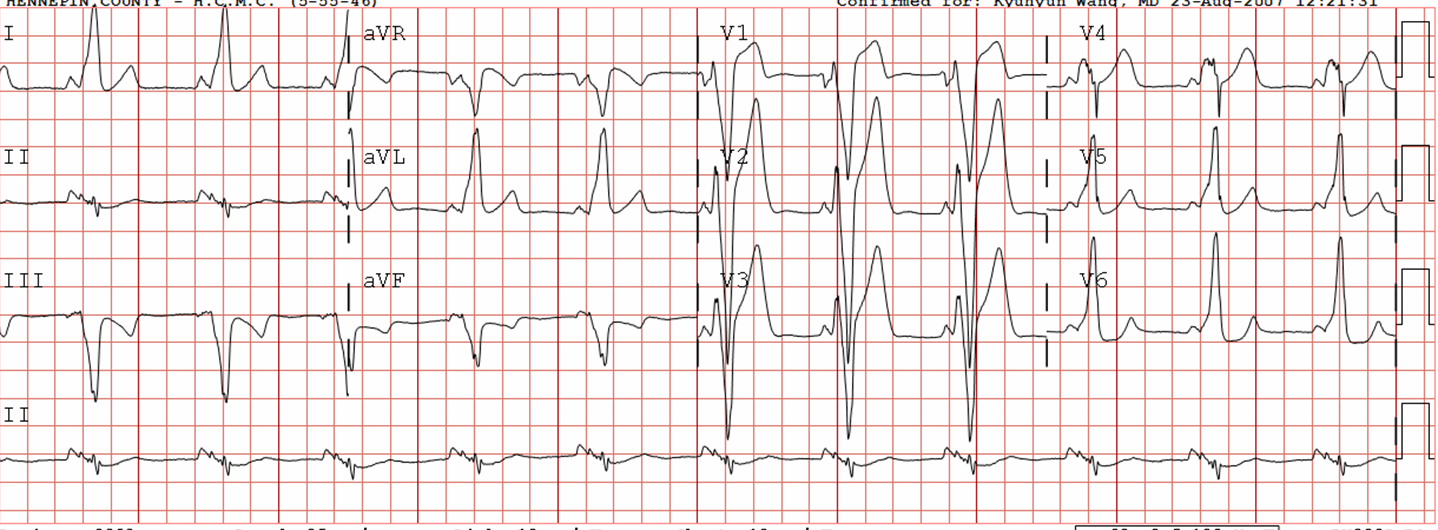
A male in his 30’s complained of sudden severe substernal chest pain. He was rushed to the critical care area where they recorded this ECG:
 |
| Obvious Antero-lateral STEMI due to proximal LAD occlusion (proximal because it is proximal to first diagonal, resulting in high lateral STEMI with ST elevation in I, aVL and reciprocal ST depression in inferior leads) |
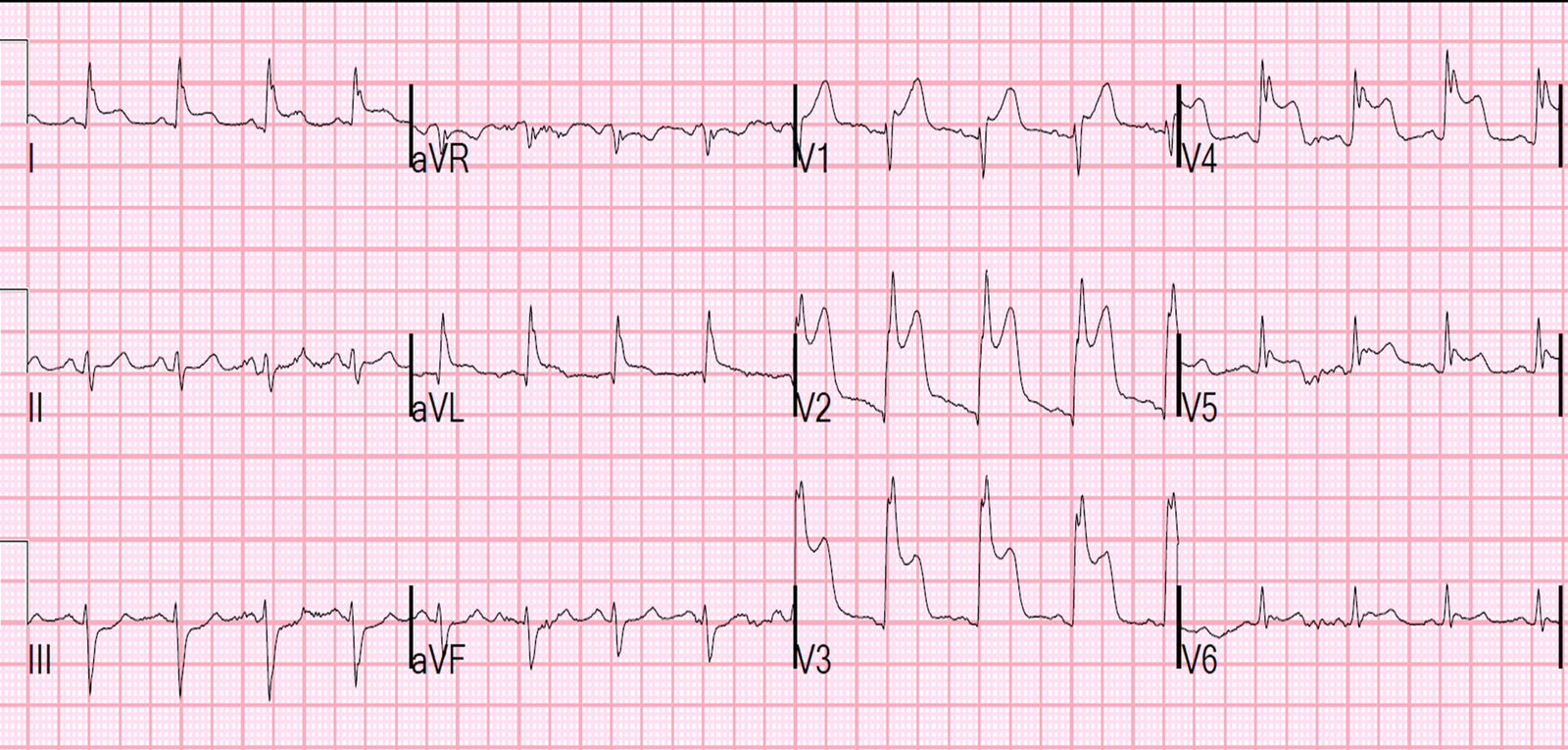
The cath lab was activated, and just before going to the cath lab (19 minutes after the first ECG), this ECG was recorded:
 |
|
|
I have often wondered if de Winter’s T-waves really are due to complete occlusion, or to severe, subtotal occlusion. Perhaps they indicate an open artery with minimal flow and severe subendocardial ischemia, but not total subepicardial ischemia.
Since ACS is so dynamic, with thrombi forming and lysing continuously, and because the ECG and angiogram are rarely simultaneous, it is probable that de Winter’s T-waves are recorded in a window when the artery is barely open.
At cath, there was a 99% lesion with some flow.
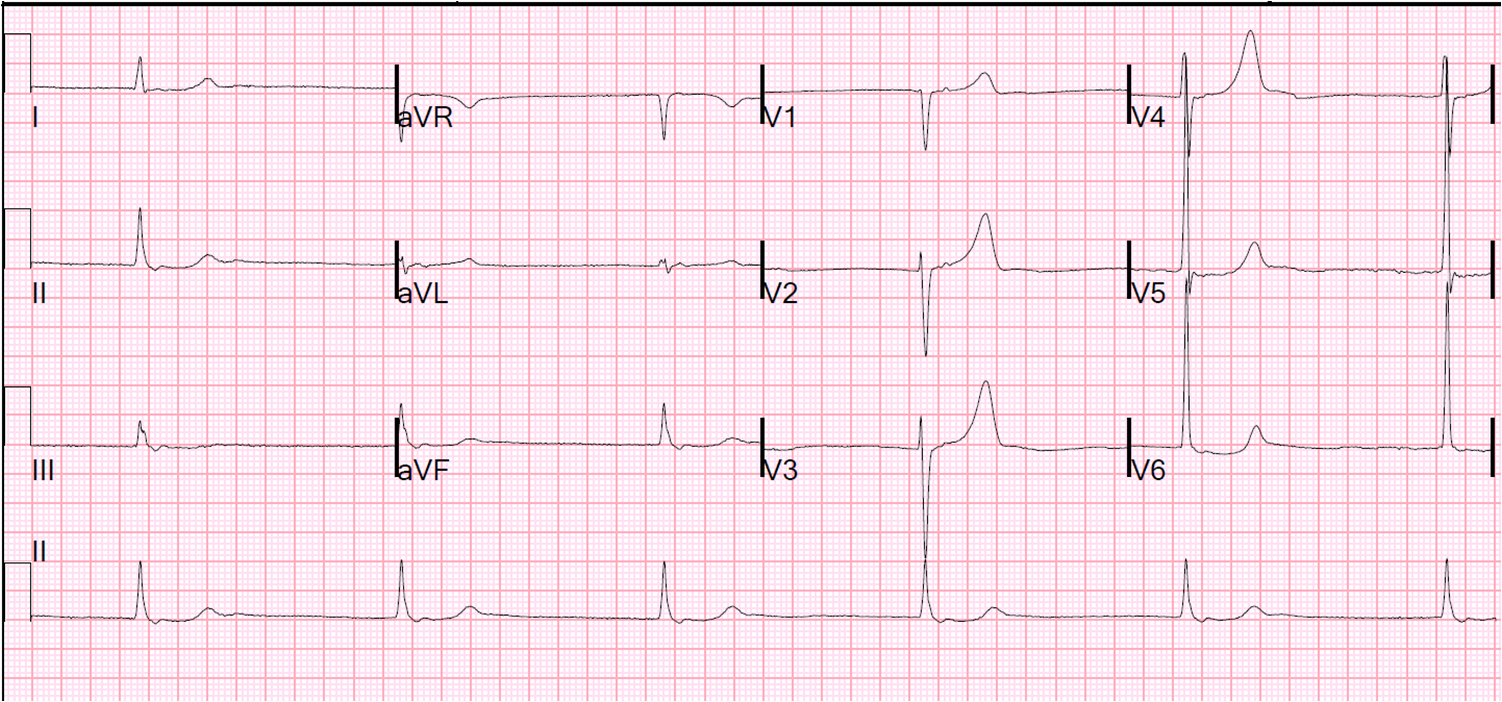
Here is the first post cath ECG, shortly after opening.
 |
| (QTc = 383). Now there are very subtle Wellens waves |
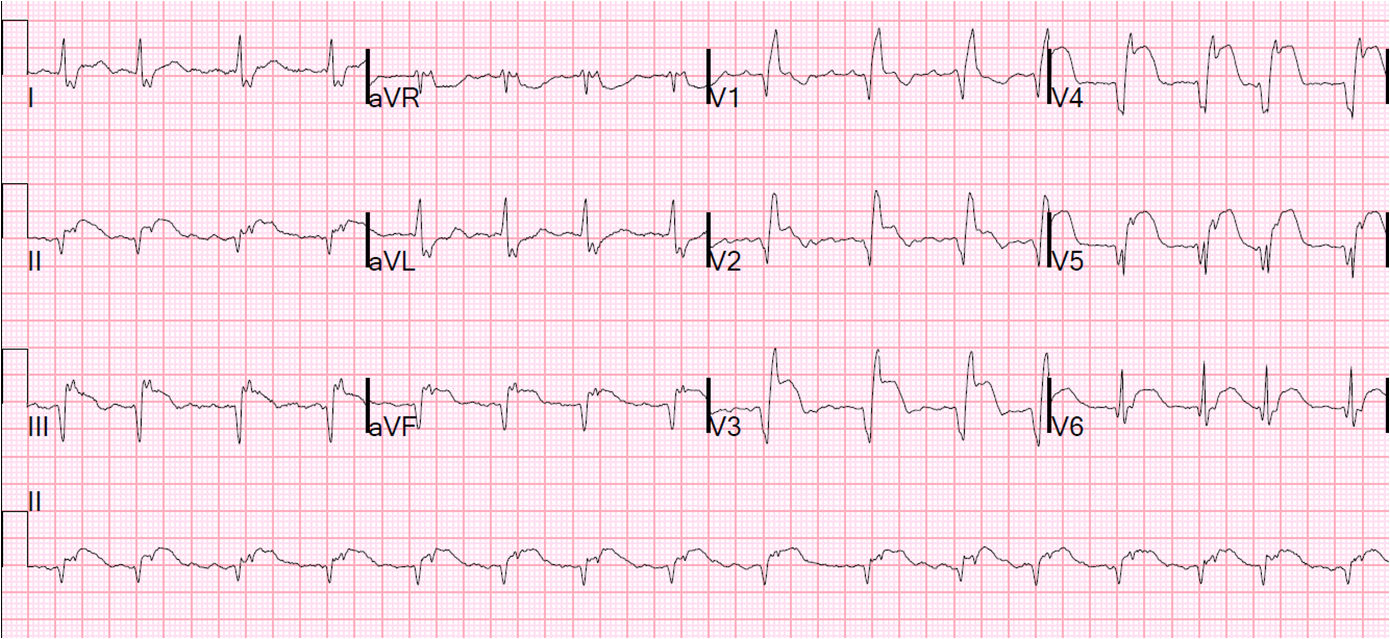
Here is the ECG the next day:
 |
| QTc 440. Well developed Wellens’ waves (reperfusion T-waves after opening of LAD occlusion) |
de Winter’s waves
de Winter et al. (Heart 2009;95:1701–1706, http://dare.uva.nl/document/214264) published on 1890 patients who had LAD occlusion. They found these “de Winter’s waves” (ST depression in V1-V6 with upsloping ST depression and a hyperacute T-wave) in 2% of these patients, and stated they were “persistent.”
A quote: “We have observed this pattern as a static ECG pattern lasting from the time of first medical contact until the recording of the pre-procedural ECG and lasting until angiographic establishment of an occluded LAD artery (that is, approximately 60 minutes)”
They gave as an example a patient with chest pain of 91 minutes who had this pattern. He had an ECG 71 minutes later and the pattern continued. Then, they say: “The coronary angiogram performed shortly after this registration revealed a fresh occlusion of the proximal LAD artery.” It is in my view that it is very likely that the artery was barely open while the de Winter’s waves were present, and closed off entirely by the time of the angiogram which was done “shortly after” the ECG.
My interpretation of this data
de Winter’s waves are probably due to severe subendocardial ischemia, with some epicardial ischemia (enough to result in hyperacute T-waves, but not enough for ST elevation.
This is somewhat academic, because these patients clearly need reperfusion whatever the exact thrombotic state of the artery.