A very healthy woman in her 20’s (who, however, is a heavy smoker) presented with 4 days of waxing and waning substernal chest pressure radiating to the throat and both shoulders. It was not sharp, not pleuritic. There were no myalgias, no viral symptoms, no F/C/S.
Looking at her, she was the picture of health, and I thought to myself: “Is there any possible way she could have an MI?”. My answer, of course was yes.
I’ve seen it too often before in young women, as for instance:
in this case, and
in this case, and others.
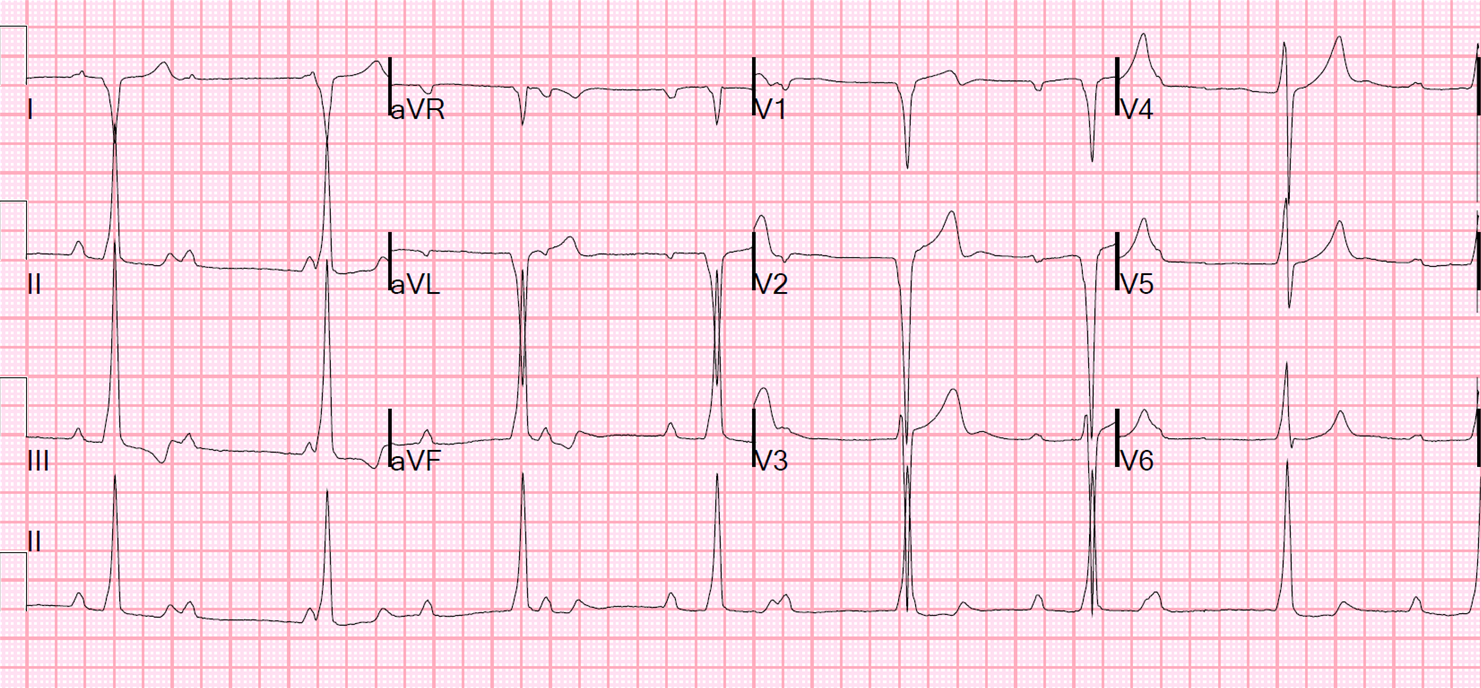
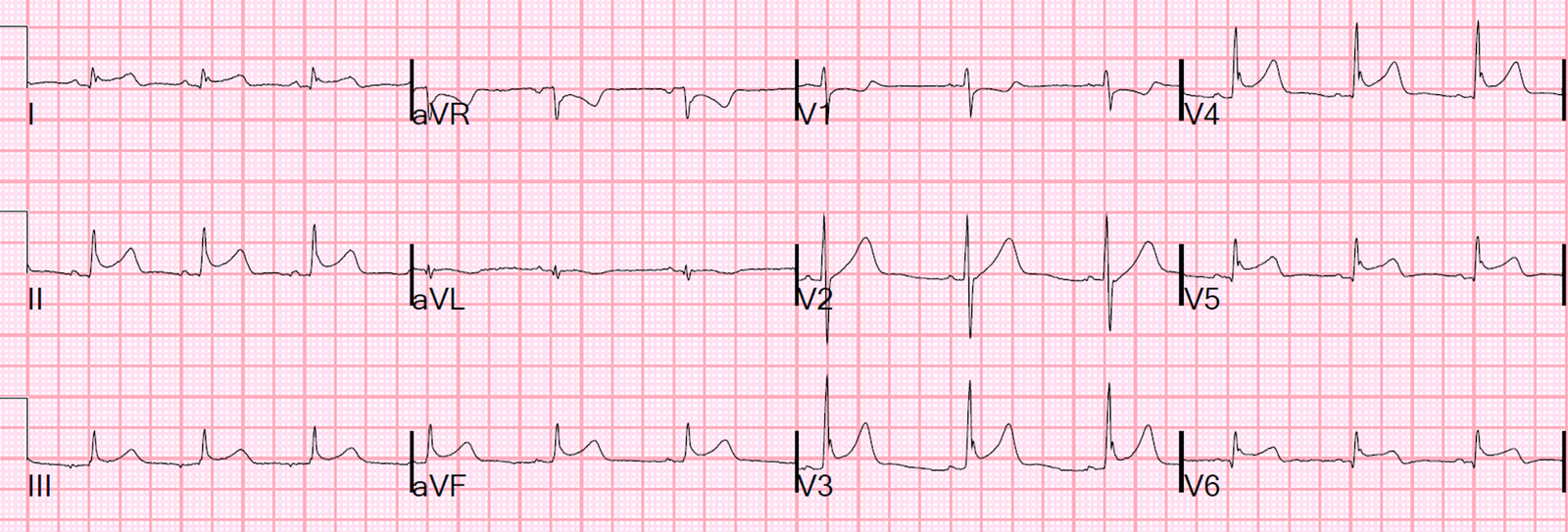
So we ordered an ECG, of course:
 |
|
I found this very interesting and worrisome. –The most obvious is ST elevation is in V3-V6. –However, there is another finding which had me very worried: ST –There is PR depression that is within normal limits –The ST elevation in aVL is only 0.5 mm, but the |
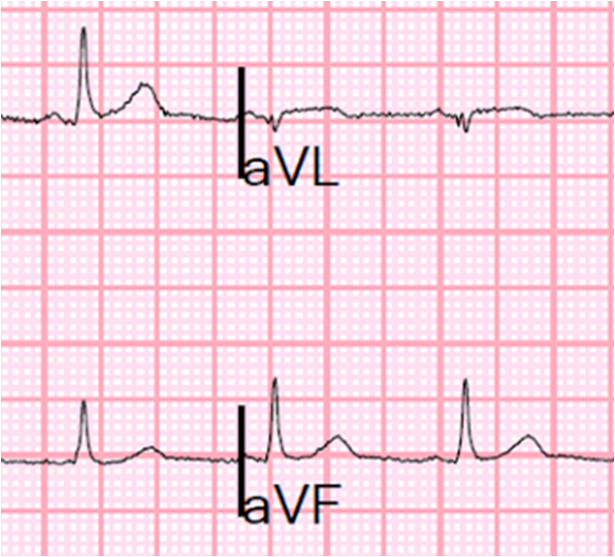
Let’s look at III and aVL enlarged:
 |
| Notice the QRS voltage is less than 0.2 mV (less than 2 mm) in aVL, and the ST segment is nearly 1 mm. So the proportional ST elevation is quite high. This is only partly due to the difference in axis between the QRS and ST segment. QRS axis is 60 degrees, towards lead II, and the ST axis is 0, towards lead I. |
Pericarditis almost never has reciprocal ST depression anywhere. If this is inflammatory and there is evidence of focality (with STE in aVL and reciprocal ST depression in III), then it is almost certainly myocarditis, as pericarditis is generally diffuse, with diffuse STE and STD found ONLY in aVR.
wall.
Focal pericarditis is unusual, but focal myocarditis is not. Pericarditis is electrocardiographically diffuse, with an ST vector towards leads II and V5 and no reciprocal ST depression except in aVR.
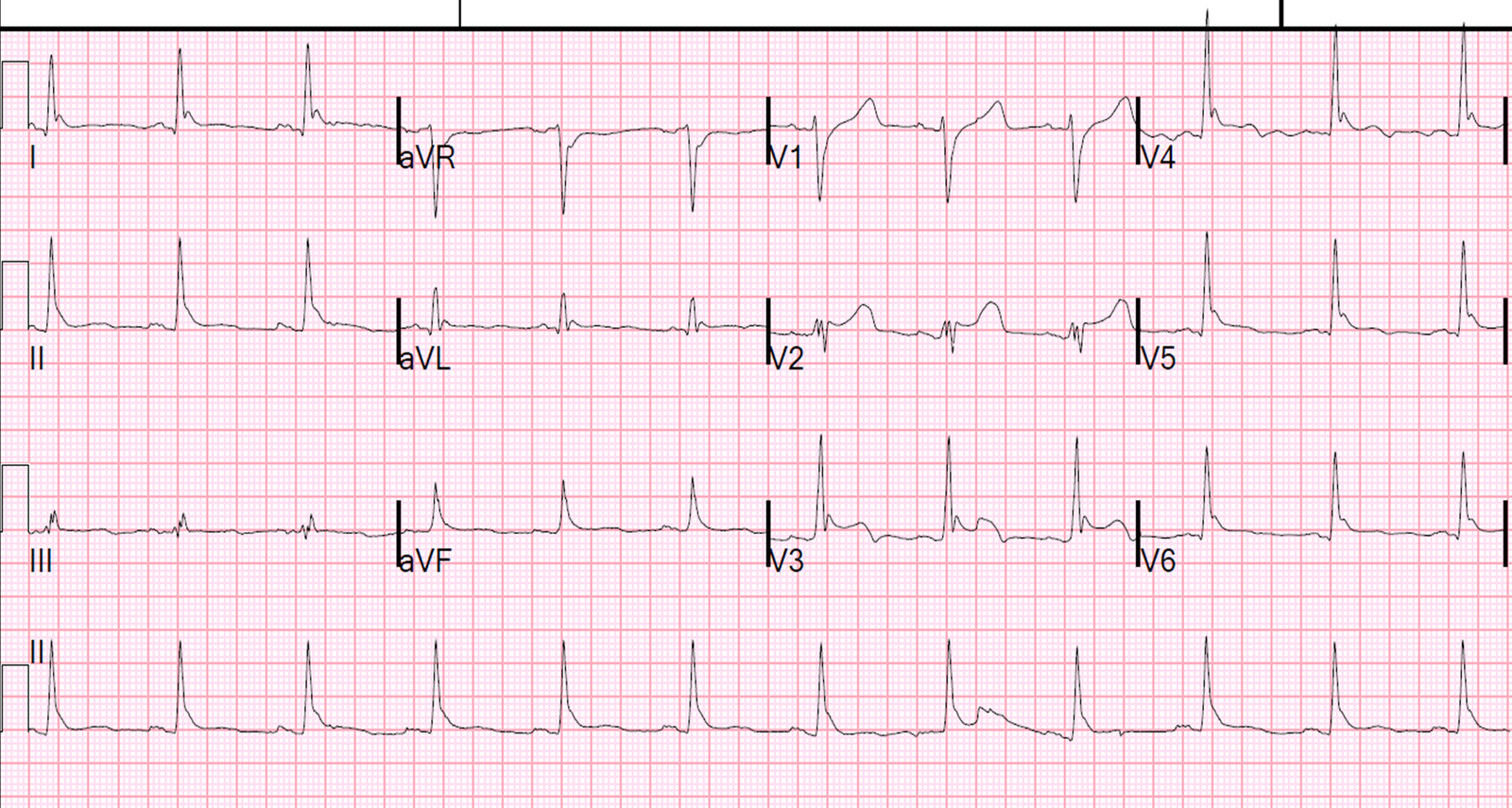
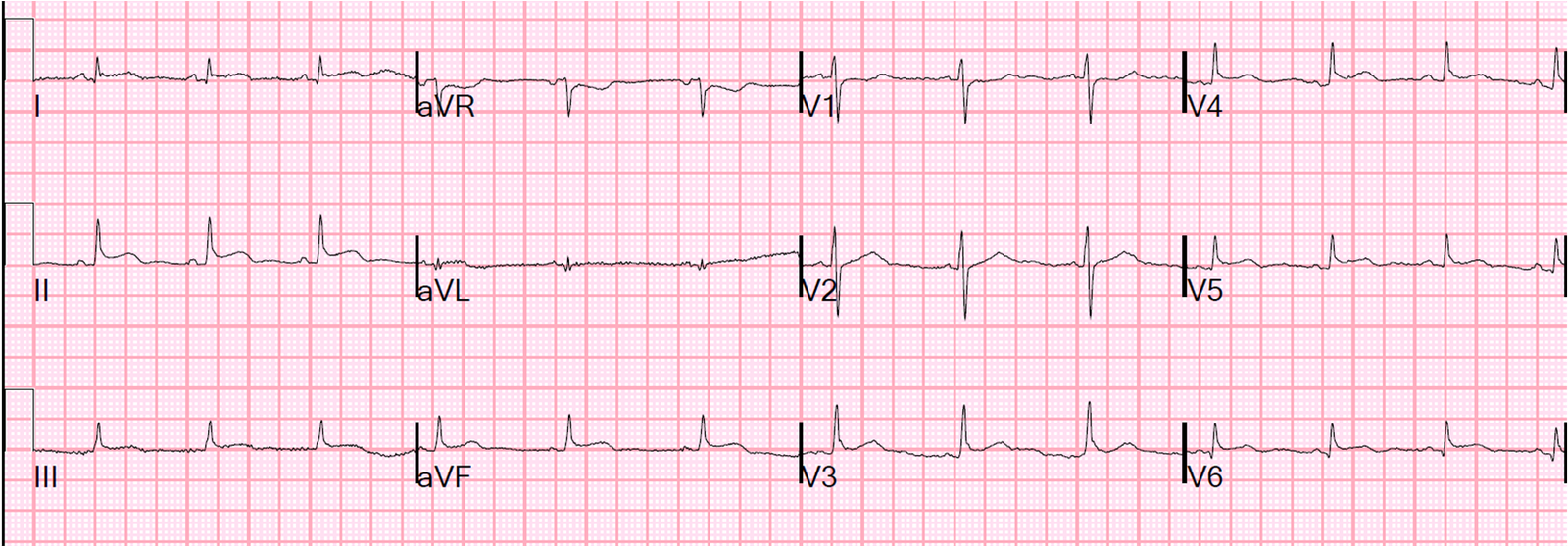
A bedside echo was normal. Troponin I was sent. Chest X-ray was normal. She was given aspirin and sublingual nitroglycerine, and her pain subsided slightly. Another ECG was recorded:
 |
| The ST deviation is less. Thus it is dymamic, which is not usually associated with myo-pericarditis, but probably because serial ECGs are not frequently obtained for this condition. |
Here is the enlargement:
The troponin I returned at 18.9 ng/mL.
Is it MI or myocarditis?
Of 45 patients, 35 had myocarditis by Indium scintigraphy (unfortunately, I don’t know how accurate this test is, and it seems that no diagnostic test is terribly accurate for myocarditis. Even the reference standard, endomyocardial biopsy, often misses the involved myocardium).
–Half of them had focal myocarditis and half diffuse.
–-28% had reciprocal ST depression.
–62% had regional wall motion abnormalities.
— In the U.S. Myocarditis treatment trial, 89% of these highly selected patients (not ED patients) had a syndrome consistent with a viral prodrome.
Thus, unfortunately, if there is a wall motion abnormality, one is really unable to differentiate acute MI from myocarditis in the emergency department.
Case Progression
I consulted our cardiologist, who sent his echo tech, and we obtained a high quality, Definity contrast echo. This was done and showed a lateral wall motion abnormality.
So we activated the cath lab. The interventionalist was very pleased to come evaluate this young woman’s coronary arteries, agreeing wholeheartedly that you can’t “sit on” someone all night who has chest pain and a positive EKG and troponin.
The angiogram was completely normal.
The left ventriculogram showed a dense lateral regional wall motion abnormality, very highly suggestive of focal myocarditis.
Serial troponin I went from 18.9 ng/mL, to 19.7 at 6 hours, to 16.8 at 9 hours, to 16.1 at 24 hours to 11.5 at 42 hours.
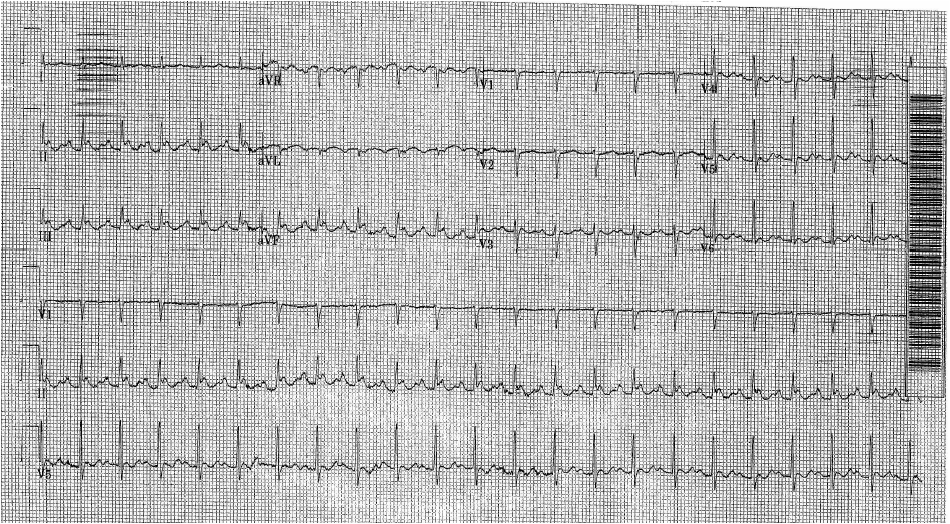
An ECG was recorded the following morning:
 |
| Now there is much more widespread ST elevation, with no reciprocal ST depression. This is classic myopericarditis. |
An MRI of the heart confirmed inflammation of the lateral wall, all but diagnostic of myocarditis.
She was treated with colchicine and ibuprofen.
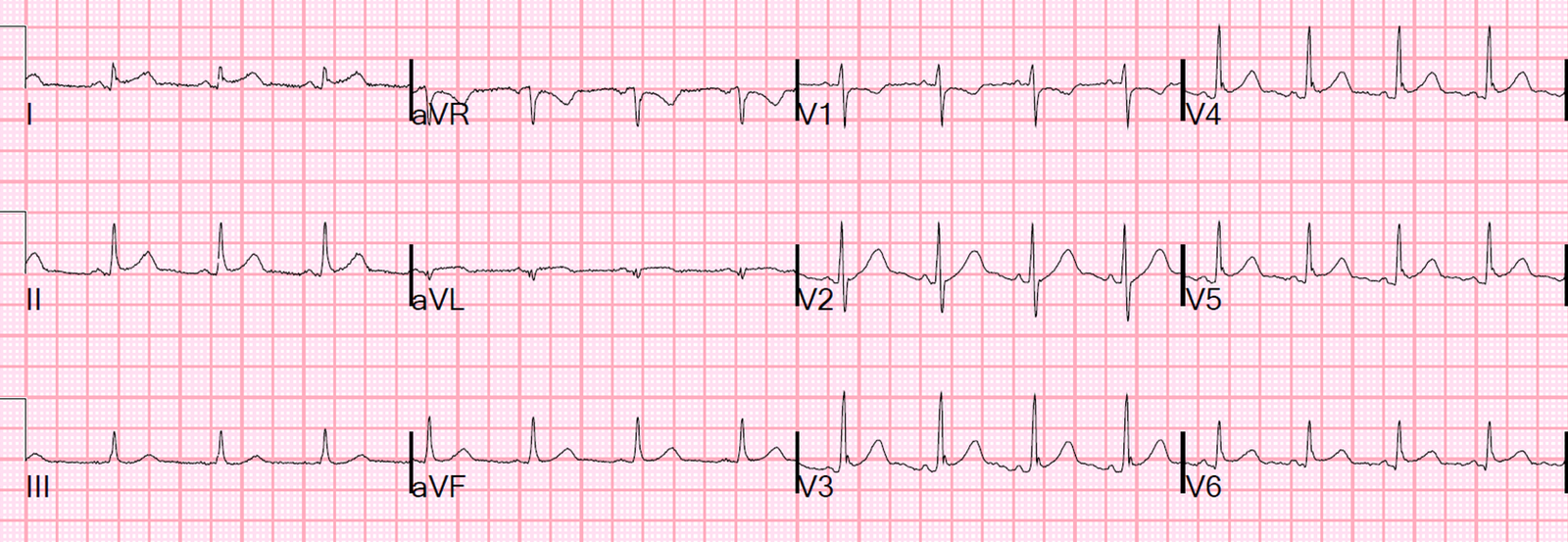
A final ECG at 42 hours was resolving:
Learning Points:
When the differential diagnosis is myocarditis vs. acute MI, it is difficult to make any conclusions without an angiogram. In half of myocarditis, there will be a wall motion abnormality (focal myocarditis) and it will be impossible to distinguish from MI. If there is no wall motion abnormality, one can be reasonably confident that it is diffuse myocarditis and avoid the emergent angiogram.
I am not at all troubled by activating the cath lab to be certain that she was not having a coronary thrombus. It put everyone’s mind to rest.