This patient in her 40’s with type 1 DM presented with 16 hours of vomiting (x 10) and diarrhea (liquid/loose x 10). She came to triage complaining of “food poisoning.” There was some diffuse abdominal pain, but no chest pain or shortness of breath. She was tachycardic to 120 and had no Kussmaul respirations. Her abdomen was diffusely tender but without guarding.
The intern presented the patient and a plan to check a chemistry panel, and to give antiemetics and fluids.
I said: “you better order an EKG; you never know when a vomiting patient, especially a diabetic, is having an MI.”
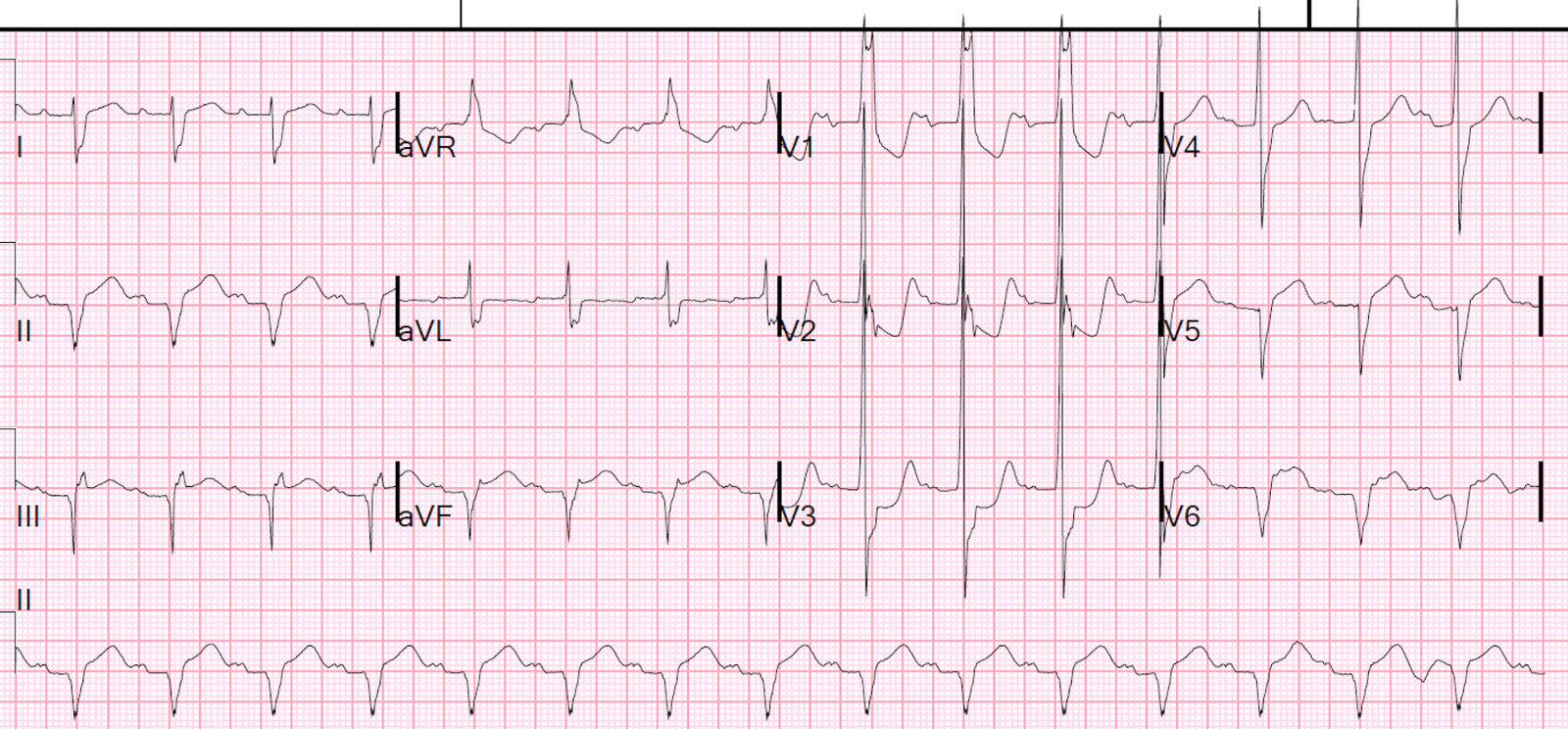
Here is her ECG:
 |
| There is anterolateral ST elevation, with well-formed QS-waves in V1-V3. This is diagnostic of a subacute anterolateral STEMI. |
She did have a mild ketoacidosis as well.
At angiography, there was a 100% thrombotic occlusion of the mid (not proximal) LAD and had evidence of prolonged occlusion (subacute MI). The initial troponin I was 88 ng/mL (88,000.00 ng/L), confirming prolonged occlusion and large MI. The highest troponin, after artery opening, was 222 ng/mL. Echo showed EF of 12% and multiple wall motion abnormalities. Angiogram showed severe downstream microocclusion.
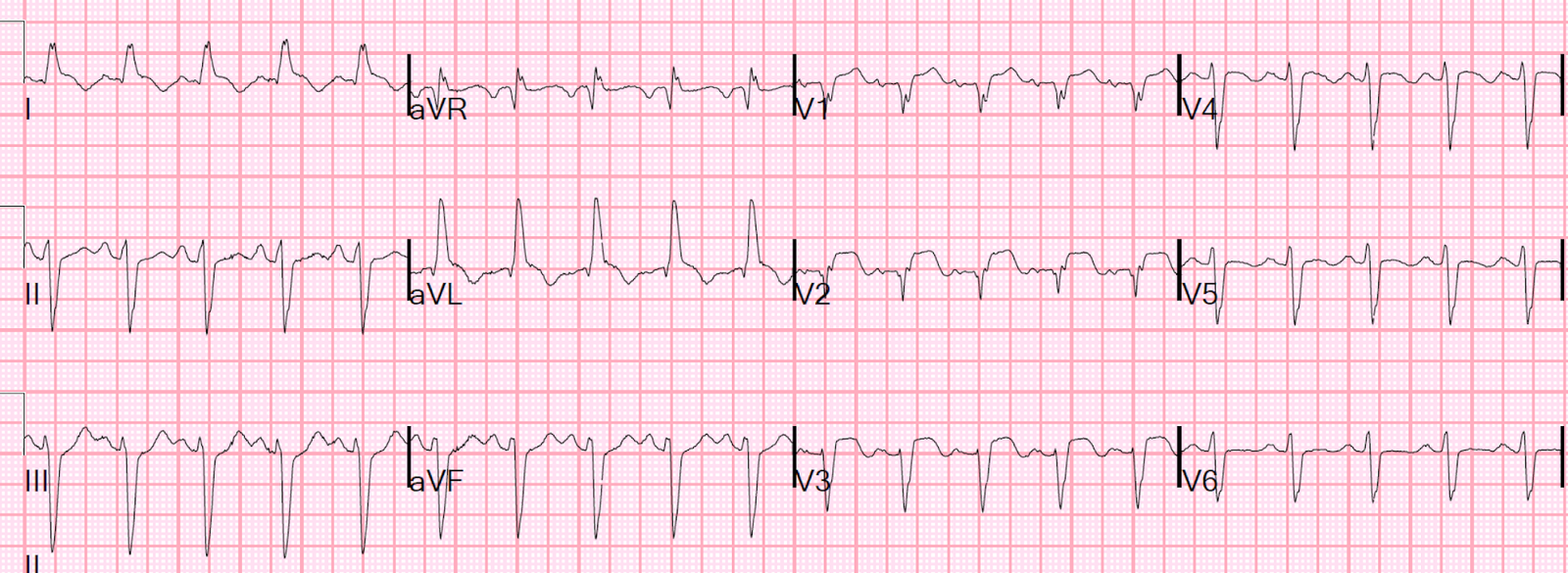
Next day ECG:
 |
| Persistent ST Elevation and Long QT. Such persistent ST elevation with QS-waves is associated with mechanical complictions (e.g., myocardial rupture) and with development of LV aneurysm. |
At 48 hours:
 |
| ST Elevation remains persistent |
Learning Points:
1. ECGs are cheap and noninvasive. As long as you know how to keep from over-interpreting ECGs in patients with a low pretest probability, it can’t hurt to order one in nearly any patient who has acute chest or abdominal symptoms.
2. A clearly diagnostic ECG is diagnostic even when there are no clearly ischemic symptoms. It may even be diagnostic when the patient has no symptoms!
Here is a case of a patient whose only symptom was hand numbness: