This was contributed by Rohin Francis (Twitter: @MedCrisis), a cardiologist from England and FOAM enthusiast.
Case
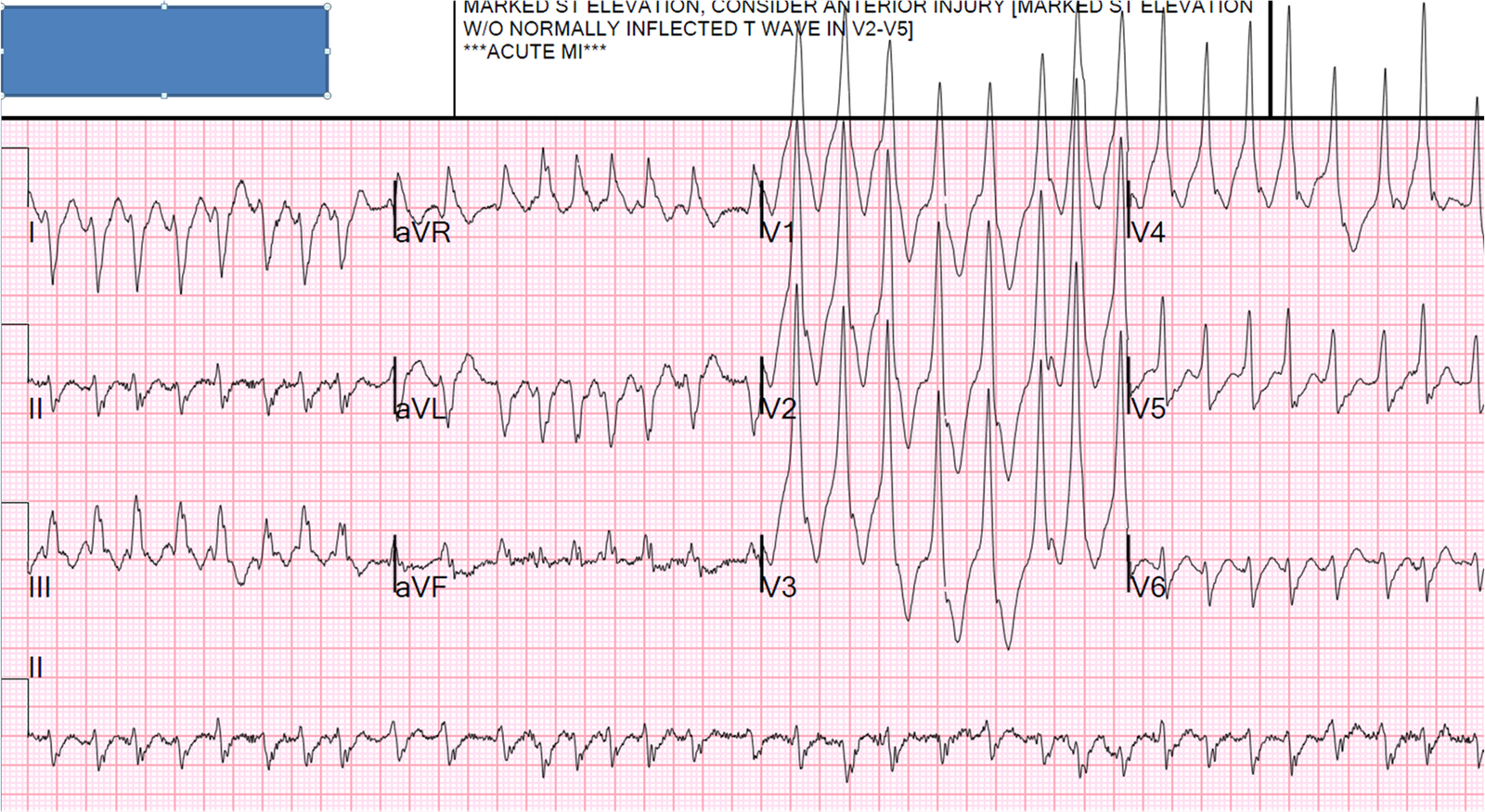
A 55 year old lady initially presented to hospital with an acutely ischaemic arm. An embolic occlusion of her brachial artery was diagnosed by CT and treated with anticoagulation. The following day she developed sudden severe chest pain. This ECG was obtained:
 |
| Sinus rhythm. The rather alarming appearance of the QRST may be mistaken for a broad complex QRS but, in fact, her QRS complex can be clearly seen in V2, V3 and II and is narrow. What has manifested as triangular complexes is actually huge ST segment elevation seen in V2-5 and laterally in I and aVL. There is also ST segment depression inferiorly. A proximal LAD occlusion can produce anterolateral ST elevation, but if the circumflex is also occluded, it is possible the anterior ST elevation might be attenuated and indeed here the ST elevation is less pronounced in V2 and V3. Smith comment: Note there is ST depression in aVR, a true sign of Left Main occlusion. Many authors state that ST elevation in aVR is a good ECG sign of left main occlusion. This is erroneous. (See this post for more explanation).
Lead aVR is opposite an imaginary lead between leads I and II, often called (-aVR). You can see that left main occlusion causes high lateral STE (aVL) with reciprocal STD (leads II and III); since aVR is reciprocal to this ST elevation, there is ST depression in lead aVR. |
Case continued
She was immediately transferred to the primary PCI centre. On
arrival she was in cardiogenic shock and haemodynamically unstable. Her
BP was 80 systolic, GCS 13 and she had a grey appearance.
An
intra-aortic balloon pump was inserted first and the cardiac arrest and
ECMO teams were alerted. This was the initial shot of her angiogram:
 |
| The guide catheter was deliberately not engaged with the left main artery, as an occlusion was suspected. Here one can see contrast being injected towards the left main and a large thrombus sitting at the ostium. A small amount of flow is passing but not reaching further than proximal circumflex nor LAD. There is sluggish clearance of contrast from the aortic root indicative of poor cardiac output. An intra-aortic balloon pump can be seen inflating and deflating in the descending aorta.Smith comment: There is near total obstruction of the Left Main. I am no angiographer, but I believe that this is TIMI-1 flow, which results in ST elevation. It is not TIMI-0 flow (total obstruction/occlusion), as some minimal contrast gets through. All thrombi are dynamic, however, and the only certainty one can have about the condition of the artery 45 minutes earlier, during recording of the ECG, comes from ECG analysis. Passing angioplasty wires into her coronary arteries restored flow to |
Here is the aspirated thrombus:
 |
| Large red thrombus aspirated |
Despite revascularisation and inotropic support, she remained in
cardiogenic shock. An on-table echocardiogram revealed severe global
impairment of her left ventricle. She was shocked out of VF on several
occasions but continued to arrest so was placed onto femoral VA ECMO.
Peripheral
ECMO increases afterload by introducing blood into the aorta and if
there is no cardiac ejection, it can cause dilatation of the LV.
Unfortunately despite maximal therapy in ICU, she continued to
deteriorate.
A trans-oesophageal
echocardiogram revealed extensive thrombus in the aortic root and left
ventricle. She died later that day. A post mortem was not performed but
disparate embolic events in her arm and coronary circulation might point
to an intra-cardiac source of thrombus. Thrombi tend to form in
impaired ventricles, but it is unclear if the severe left failure seen
on echo was pre-existing or simply a result of a catastrophic acute
coronary syndrome.