
Written by Meyers, edits by Smith
A 50-ish year old man was working construction when he suddenly collapsed. Coworkers started CPR within 1 minute of collapse. EMS arrived within 10 minutes and continued CPR and ACLS, noting alternating asystole and sinus bradycardia during rhythm checks. He received various ACLS medications and arrived at the ED with a perfusing rhythm.
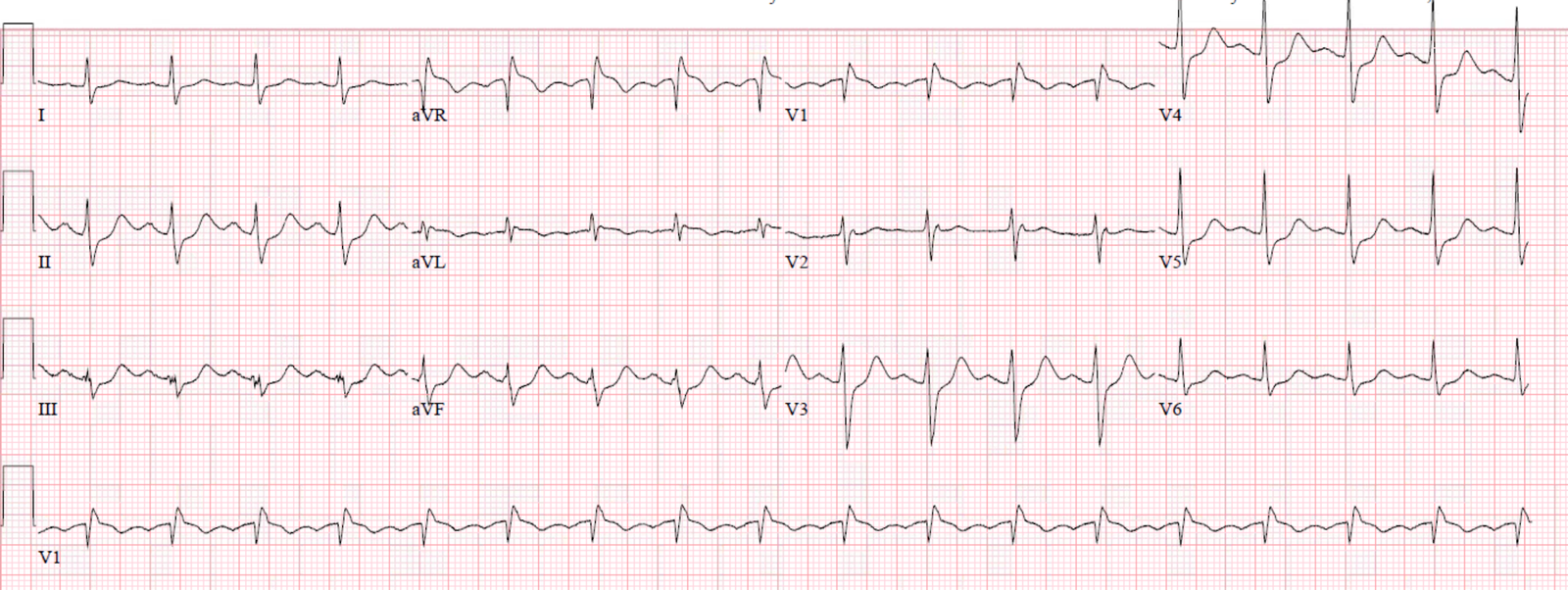
Initial vitals included heart rate around 100 bpm and BP 174/96. Here is his initial ECG, very soon after ROSC:
 |
| What do you think? |
Sinus tachycardia. There is incomplete RBBB (QRS duration less than 120 ms). There is diffuse STD, maximal in V4-V5 and lead II. There is a tiny bit of STE in aVL, and there is a significant amount of reciprocal STE in lead aVR, and less so in V1.
Comment/Refresher on Lead aVR:
Remember: think of lead aVR this way: “aVR = the aVerage Reciprocal lead to the rest of the ECG”. There is no wall of the heart that corresponds to the direction of lead aVR, but rather it is the opposite direction of the main average vector of depolarization and repolarization of the heart, opposite leads V4-V6 and lead II. It is not really possible to have Occlusion MI that affects a myocardial wall and causes primary STE in lead aVR. Instead, lead aVR simply reflects any ECG finding which is found diffusely throughout the ECG, especially those findings which are directed opposite of it (V4-V6 and lead II).
Thus, anything that causes widespread STD will always come with STE in aVR, and the differential of widespread STD is enormous, including any process that causes diffuse supply/demand mismatch but NOT complete lack of blood flow (as seen in Occlusion MI with no collateral circulation). One of the rarest causes of this pattern would be acute but non-occlusive left main ACS (or any single vessel ACS in the setting of preexisting triple vessel disease), which of course would benefit from emergent angiography and intervention. However, non-ACS causes are by far more common overall.
See our many other posts on aVR for more details.
Among other considerations in this case is whether this arrest was caused by ACS. As above, widespread STD with STE in aVR has many etiologies, not just ACS. If the arrest itself caused ischemia, then stabilization and supportive care may lead to resolution, so serial ECGs remaining ischemic support ACS, while those which resolve generally support another etiology (however, of couse, even ACS is dynamic, with thrombus propagating and lysing, so an improving ECG may just be lysis of a thrombus that could later re-propogate from that ruptured, exposed plaque.)
Also, the circumstances of the arrest are a strong clue to etiology. A shockable rhythm is far more likely to be due to ACS than a non-shockable rhythm, which is what we appear to have here.
Case continued:
The team recognized the diffuse STD and decided to repeat it every 5-10 minutes while stabilizing the patient and assessing for any other modifiable factors to explain diffuse supply/demand mismatch.
Here is the ECG 10 minutes after sustained ROSC and normal-to-high blood pressure (without any continued vasopressors needed).
 |
| Similar findings, but slightly less pronounced. |
They got another repeat ECG 15 minutes later:
 |
| Continued diffuse STD with obligatory STE in aVR. |
It has now been at least 25 minutes with continued ROSC and reasonable vital signs, and the diffuse STD with reciprocal STE in aVR have persisted despite no clear reversible reason for increased demand or indequate coronary perfusion. Thus, the wide differential has narrowed significantly, and ACS is still on the differential since we have not found any other reversible reason for supply demand mismatch.
The team considered activating the cath lab for these ongoing ECG findings despite resuscitation.
However, they also noticed minimal signs of neurologic activity despite short low-flow time, and began to suspect a possible intracranial source.
So before activating the cath lab they took the patient for a head CT, which showed:
 |
| Massive subarachnoid hemorrhage. |
The patient did not undergo cath, and ultimately expired.
Here is another case written by Smith:
I saw this patient many years ago: She was a 40-something year-old woman who suddenly collapsed at a bus stop. Medics found her comatose and in VT. She was cardioverted and brought to the ED with a GCS of 3.
 |
| Looks like a high lateral STEMI with STE in V2-V6, I, and aVL. Because there is widespread STE, aVR must show some reciprocal STD (because aVR = aVerage Reciprocal).
Is this a STEMI? |
What bothered me was that she had become instantaneously comatose from VT. Such immediate coma is of course common with VF, but not VT. Furthermore, she was quickly resuscitated and remained a GCS of 3.
Therefore we scanned her head and she had a lethal intracranial hemorrhage.
It was NOT a STEMI. It was stress cardiomyopathy from intracranial hemorrhage.
Learning Points:
Lead aVR = the aVerage Reciprocal lead to the rest of the ECG
Diffuse STD which is maximal in V4-V6 and lead II, MUST come with reciprocal STE in aVR, and this represents diffuse supply/demand mismatch, for which the differential is enormous but does rarely include ACS which may benefit from emergent reperfusion. The key to distinguishing these rare patients with STE in aVR who need emergent cath lab activation is:
1) First make sure that the patients symptoms and presentation are consistent with ACS.
2) Make sure that you identify and correct all reversible non-ACS causes of increased demand (atrial fibrillation with rapid ventricular rate, increased afterload from extreme hypertension, aortic stenosis, ICH, etc) or decreased myocardial oxygen supply (hypotension, hypoxemia, anemia, etc.)
3) If no other clear source of supply/demand mismatch can be found or corrected, then ACS is a likely cause of decreased supply and the patient may benefit from emergent cath.
4) Non-shockable initial rhythm makes it unlikely that ACS was the cause of cardiac arrest.
![]()
===================================
MY Comment, by KEN GRAUER, MD (11/3/2019):
===================================
Informative post by Drs. Meyers and Smith — regarding the entity of diffuse ST segment depression that occurs in association with ST elevation in lead aVR.
- As per Dr. Meyers — the presence of these ECG findings represents diffuse supply/demand mismatch.
I limit my comments to a number of points regarding ECG findings in the initial 12-lead tracing.
- I have labeled this initial ECG as ECG #1. For clarity — I have lightened this tracing and optimized resolution in Figure-1.
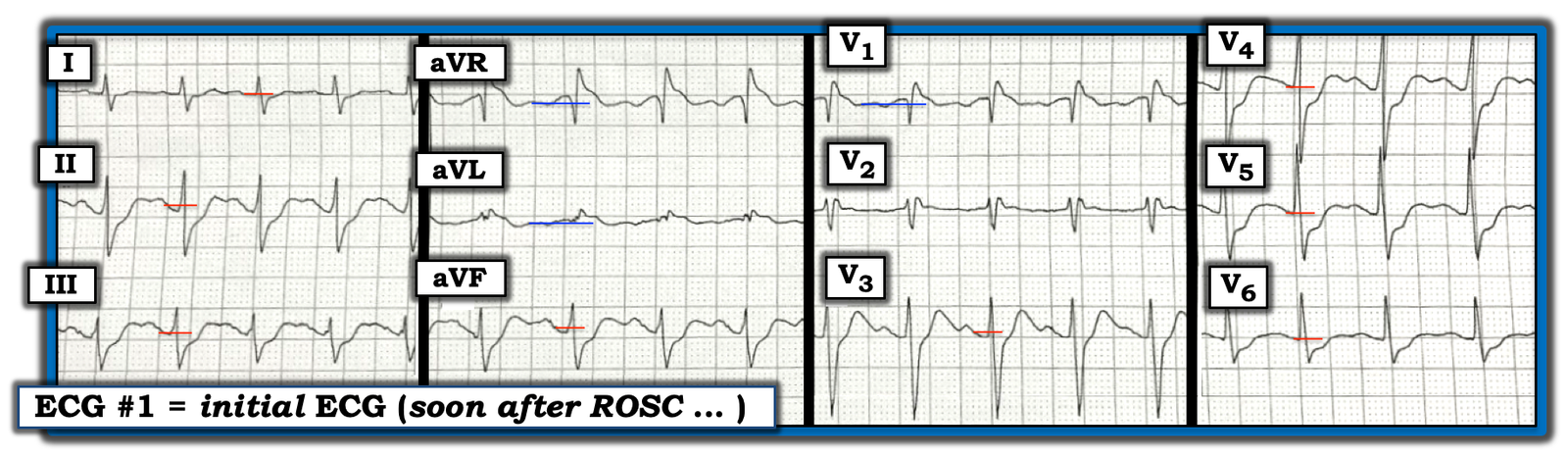 |
| Figure-1: The initial ECG in this case (See text). |
The important ECG findings in ECG #1 are the following:
- There is sinus tachycardia at ~110/minute. Regarding intervals — the PR interval looks to be normal. Although the QRS looks a little wide, I measure it no more than half a large box in duration (ie, ~0.10 second). The QTc appears prolonged, though it is difficult to precisely measure, and to assess the clinical significance of the QTc here, given the increased rate and marked ST-T wave changes.
- As per Dr. Meyers — there is incomplete RBBB because: i) there is a QR’ pattern in lead V1 (with an rSr’ in lead V2); ii) there are terminal s waves in left-sided leads I and V6; and, iii) the QRS complex is not wide enough to qualify as “complete” RBBB.
Regarding ST–T Wave Changes — the alteration in QRS morphology from the incomplete RBBB makes assessment of the amount of ST elevation and depression challenging. To facilitate this — I’ve added short colored horizontal lines in Figure-1 to illustrate what I chose as my “baseline” for assessing ST segment deviation.
- Diffuse ST segment depression is seen here in no less than 8 leads (RED horizontal lines serving as the baseline I used to assess ST depression). As per Dr. Meyers — ST depression is most marked in leads II, V4 and V5.
- ST elevation is most marked in lead aVR — but it is also seen in leads aVL and V1 (BLUE horizontal lines serving as the baseline I used to assess ST elevation).
- There is minimal ST segment deviation in lead V2 — with this being the only lead without clear ST elevation or depression.
NOTE — Opinion is divided as to whether the optimal “baseline” for assessing the amount of ST segment elevation or depression should be the PR or TP segment.
- In practice, this gets complicated — since the PR segment tends to shorten with tachycardia — PR segment depression and/or elevation may sometimes be present (this occurs not only with pericarditis! — but also with other entities, as is seen here) — there may be baseline wander (due to patient movement, tremor, pain, shortness of breath, etc.) — and, in cases like the ECG shown in Figure-1 — the limits of the TP segment are not always clear.
- While I generally favor use of the PR segment as my baseline — I always survey the entire tracing, and often end up using a combination of PR and TP segments in various leads. (CLICK HERE and watch the next 3 minutes of this ECG video — if interested in “My Take” on how I decide on the ST–T wave baseline). I acknowledge that others may differ with the baselines I chose in Figure-1 to assess ST segment deviation.
MY Preference in Terminology: Realizing that supply/demand mismatch represents the underlying pathophysiologic process responsible for the findings we see in ECG #1 — I favor use of the term diffuse Subendocardial Ischemia for the words I use to describe these ECG findings in my interpretation:
- As per Dr. Meyers — the differential diagnosis of entities that may produce diffuse subendocardial ischemia is large. It includes tachycardia, severe anemia, septicemia, hypoxemia, shock, serious arrhythmias, cardiac arrest, “sick patient”, and significant underlying coronary disease, to name a few.
- The History is KEY for suggesting the most likely cause(s) for the case at hand. Significant coronary disease (ie, multivessel, proximal LAD or LMain disease) — is not rare under the right clinical circumstances.
- The case presented here is different — as this 50-ish year old man had sudden collapse (without preceding chest pain) — the initial rhythm was non-shockable (alternating between bradycardia and asystole) — and, despite return of reasonable vital signs, neurologic activity remained severely depressed.
- The astute clinicians in this case ordered a head CT prior to activation of the cath lab — and this revealed massive subarachnoid hemorrhage. PEARL — CNS catastrophes (stroke, bleed, trauma, tumor, sudden coma, etc.) are notorious for causing among the most abnormal (and sometimes bizarre) ECG findings. Pseudo-infarct patterns are common with CNS catastrophes — and may manifest Q waves, diffuse ST segment elevation and/or depression — often with a markedly prolonged QTc. This patient’s massive subarachnoid hemorrhage with associated tachycardia, could certainly have caused the ECG picture seen in Figure-1.
- NOTE: The entity of diffuse subendocardial ischemia has been discussed on multiple occasions in Dr. Smith’s ECG Blog. I’ll simply reference the February 28, 2018 post as a nice review of this entity.
Our THANKS to Drs. Meyers and Smith for presenting this case!
![]()

