This was sent by a reader.
A previously healthy 53 yo woman was transferred to a receiving hospital in cardiogenic shock.
pH was 6.9 and K was normal.
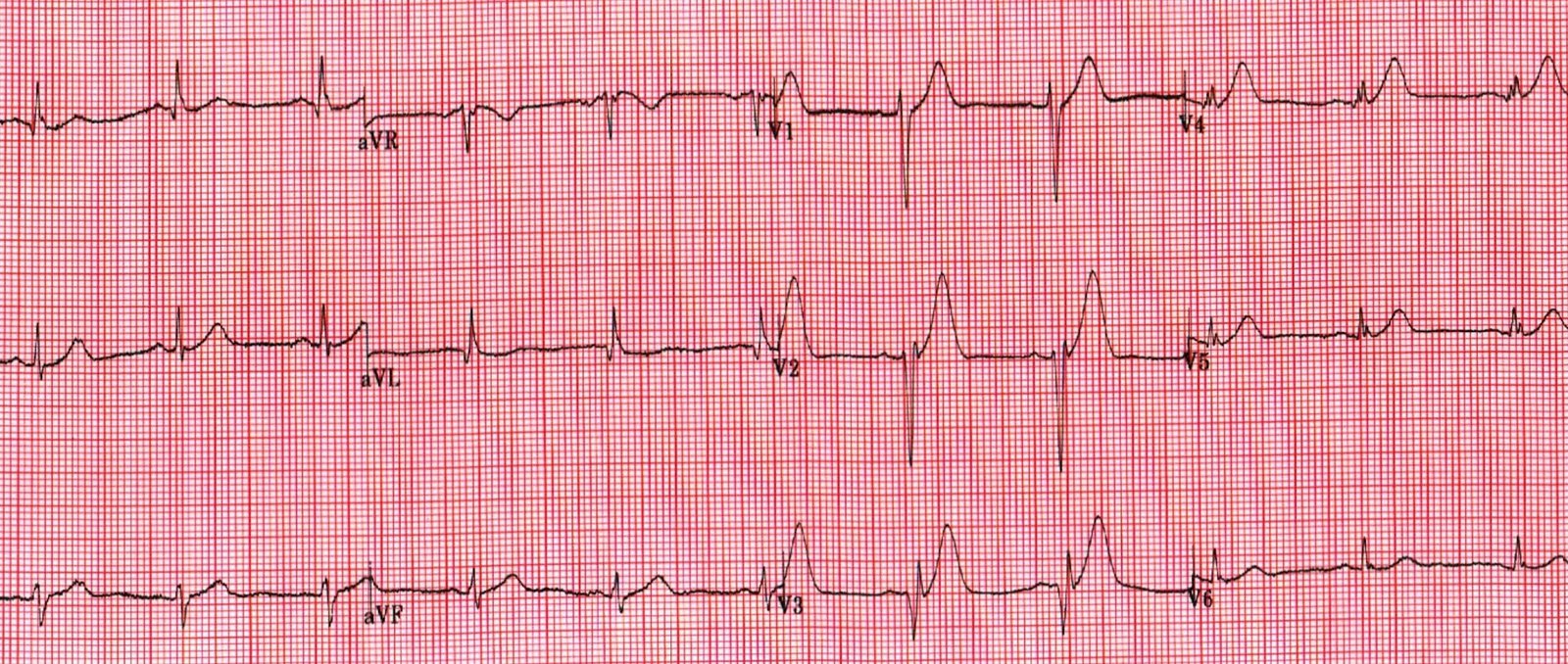
Here was the ECG:
 |
| There is sinus tachycardia. This is “Shark Fin” morphology. Shark Fin has also been called: |
Usually shark fin is in one coronary distribution and represents massive ST elevation that is as high as the peak of the R-wave and therefore fuses the R-wave and ST segment.
So Shark Fin really is just a dramatic representation of STEMI, and can be in any coronary distribution.
It is often confused with a wide QRS due to conditions such as hyperkalemia. But it is very distinct from hyperkalemia (and anything else, including VT), and such confusion can only be due to lack of familiarity, because, if you look closely, its morpholgoy is very different from anything else.
So this is STEMI, right?
Which artery?
There is ST Elevation in every lead except aVR (STD in aVR).
Well, don’t we see diffuse ST Elevation in Myo-pericarditis (with STD in aVR)? Could this be myopericarditis?
The patient was hypothermic at 90 degrees F (32.2 C) and she was positive for influenza. Her troponin I was 500.01 ng/mL (equivalent to a high sensitivity troponin I of 500,000 ng/L). This is among the highest troponin I of which I have ever heard.
Her ejection fraction was 10%.
She was taken to the cath lab and her coronaries were clean!!
There was no MRI, but the presumptive diagnosis is myocarditis.
Our chief of cardiology, Gautam Shroff, interprets it differently and thinks this is indeed ischemia. Here is what he wrote:
“This is a marker of coronary perfusion pressure in the context of severe elevated in LVEDP outside the range of coronary auto regulation. I have seen this pattern in severe acute AI also.” In other words, the severely increased end diastolic pressure from the extremely poor LV function caused by the myocarditis results in extremely poor coronary perfusion pressure.
![]()
===================================
MY Comment by KEN GRAUER, MD (2/16/2020):
===================================
As per the title by Dr. Smith — this case was not what I thought. I did recognize the Shark Fin morphology of dramatic ST elevation. Shark Fin morphology has been shown on Dr. Smith’s blog a number of times, including:
- In the June 11, 2018 post —
- In the October 4, 2019 post —
- In the November 22, 2019 post —
- in the January, 24, 2020 post —
PEARL — What I did not appreciate when I reviewed this case — was that among the many potential etiologies of acute myocarditis was HypoThermia!
- I have summarized the major etiologic categories of acute myocarditis and inflammatory cardiomyopathies. A more complete listing of specific etiologic agents can be found on the source I used to prepare Figure-1 (Kühl Uwe & Schultheiss Heinz-Peter: Myocarditis — Deutsches Ärzteblatt Int. 109 (20):361-368, 2012 — CLICK HERE).
- Referring to Figure-1 — this 53-year old woman who presented in extremis with cardiogenic shock and an initial pH = 6.9, had at least 2 potential etiologies for developing acute myocarditis: i) Profound hypothermia (core temperature = 90°F = 32.2°C); and, ii) She tested positive for influenza.
 |
| Figure-1: Potential etiologic categories of acute myocarditis (See text). |
Our THANKS to Dr. Smith for presenting this case!
![]()