A 50-something woman presented with chest pain, midsternal, 9/10.
Her BP was 93/58, pulse 110.
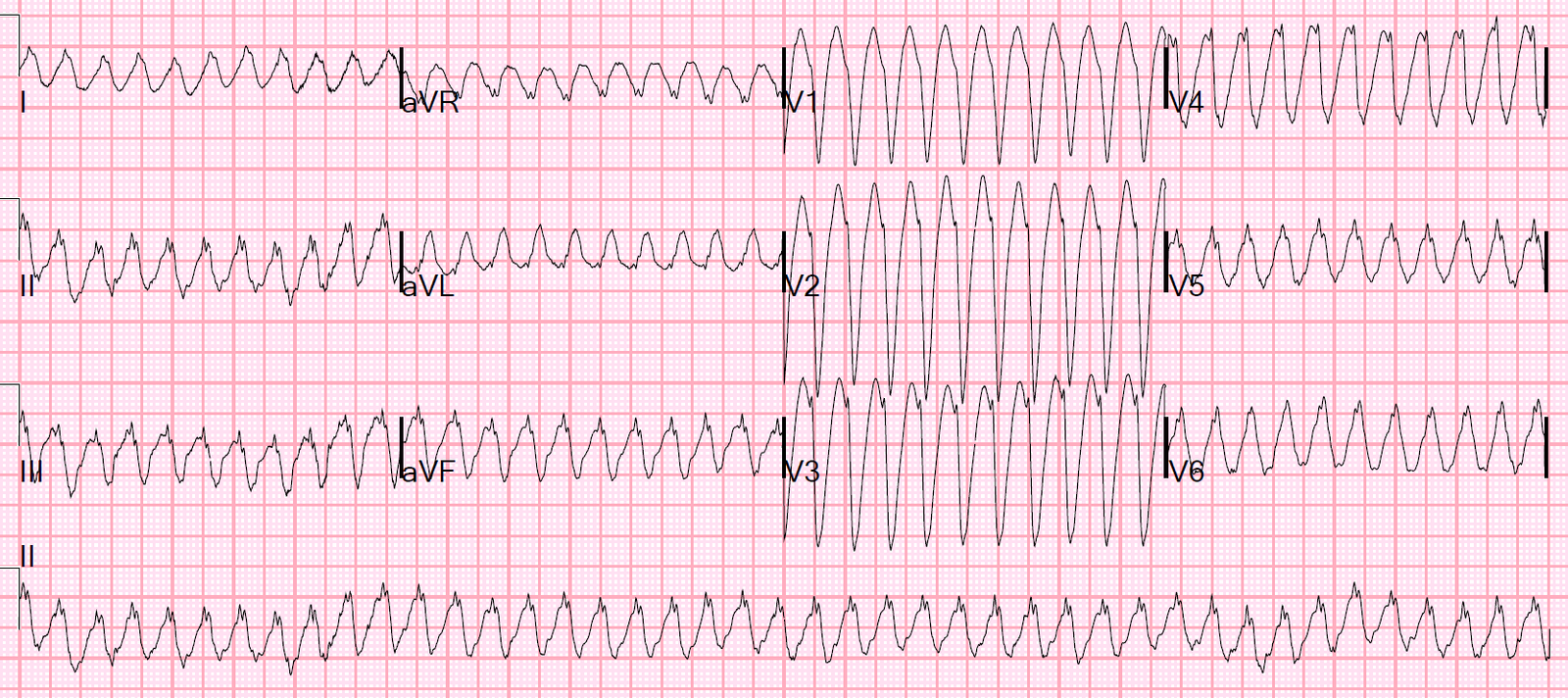
Here is her ECG:
 |
| What is the infarct artery? |
There is STE in V1-V6, maximal in V2 and quite profound in V1.
There is also STE in II, III, aVF, with reciprocal STD in I and aVL.
The differential is:
1) LAD occlusion proximal to the septal perforator with wraparound to inferior wall
(that much STE in V1 is quite specific for septal involvement with anterior STEMI)
vs.
2) Proximal RCA with RV involvement.
Is it important to know whether this is LAD or RCA?
Somewhat, but not hugely important. You would be more careful with nitro in RV infarct. You might give fluids for hypotension in either case, but in LAD you would be very worried about pulmonary edema with fluids.
Another reason it is important is that it can help the interventionalist find the culprit, as in this case:
https://drsmithsecgblog.com/2011/01/rv-mi-diagnosed-by-st-elevation-in-v1.html
How can you tell whether LAD or RCA?
First, the 12-lead:
1. The hypotension and tachycardia could happen with either. When it happens with LAD occlusion, it is usually due to poor LV function.
2. The degree of STE in inferior leads favors RCA.
3. The Maximal STE in V2 vs. V3 favors RV infarct over LAD.
4. If LAD occlusion, the STE in V1 means that it would need proximal to the septal perforator, which is also usually proximal to D1, which would cause STE in aVL and recipocal STD in III, or at least attenuate the STE in III.
Second and easiest
Record a right sided ECG — this was not done
See this case for a right sided ECG:
https://drsmithsecgblog.com/2016/01/inferior-stemi-with-av-block.html
Third and Finally
Do a bedside ultrasound.
Results of ultrasound:
1. There was no pulmonary edema (no B-lines), which supports RV MI over LAD
2. Cardiac videos below (what do you see?):
Here 2 point of care cardiac ultrasound videos to help you determine the infarct artery for this STEMI
Not great quality, but it shows a large RV
Not great quality again, but large RV
The RV (top chamber in both images) is very large. The LV function is good and the LV is small. This strongly suggests that this is an inferior and right ventricular STEMI due to a proximal RCA occlusion, NOT an LAD occlusion.
She went to the cath lab and indeed had a proximal RCA occlusion (proximal to the RV marginal branch, which supplies the RV).
Angiogram
Culprit is 100% occlusion of the proximal RCA.
Peak troponin I was 150 ng/mL (Very large MI).
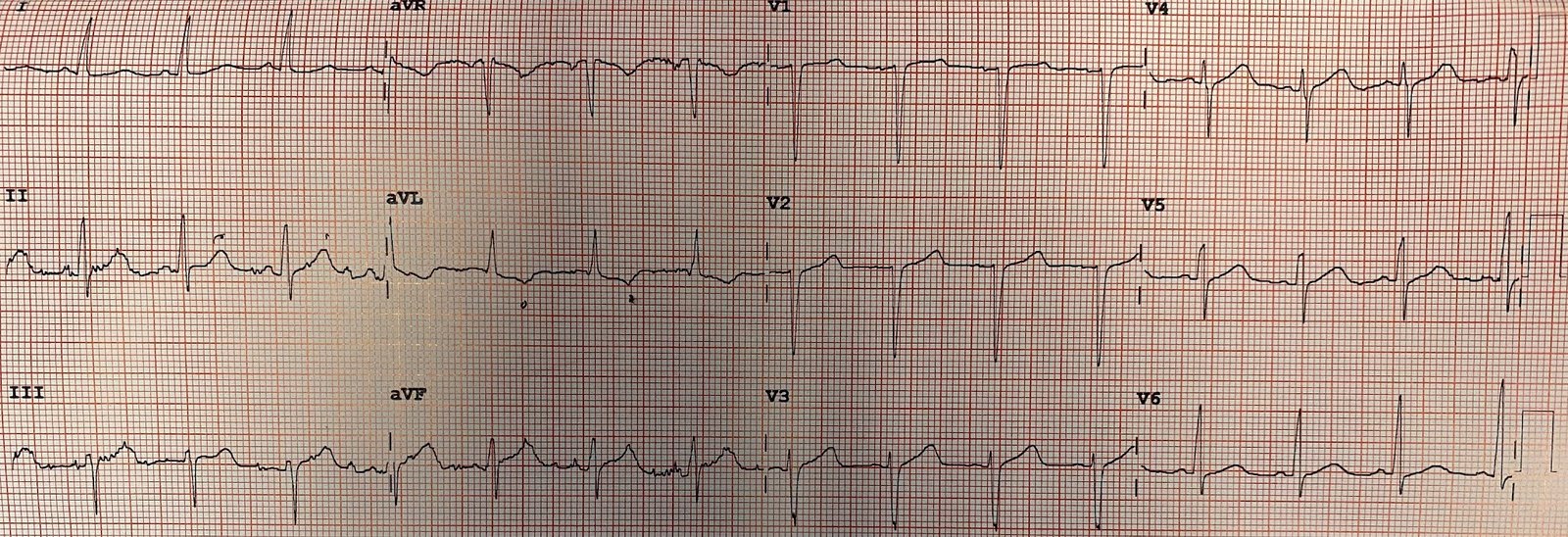
Next day bubble contrast ultrasound:
The estimated left ventricular ejection fraction is 63%.
Regional wall motion abnormality-inferior hypokinetic and small.
(There is surprisingly little myocardial damage by echo.)
![]()
===================================
MY Comment by KEN GRAUER, MD (6/6/2020):
===================================
Superb example by Dr. Smith regarding the clinical decision-making process for predicting the “culprit artery” ( = IRA = Infarct-Related Artery) when there is acute ST elevation in both inferior and anterior leads, in the special case when there is marked ST elevation in lead V1.
- KEY Point: As emphasized by Dr. Smith — Clinically, distinction between proximal LAD occlusion vs proximal RCA occlusion with acute RV involvement is of limited benefit (ie, more cautious use of NTG with acute RV involvement — given differing hemodynamics compared to anterior MI). And as per Dr. Smith — accurate prediction of the IRA could be quickly forthcoming from obtaining either right-sided leads and/or bedside Echo.
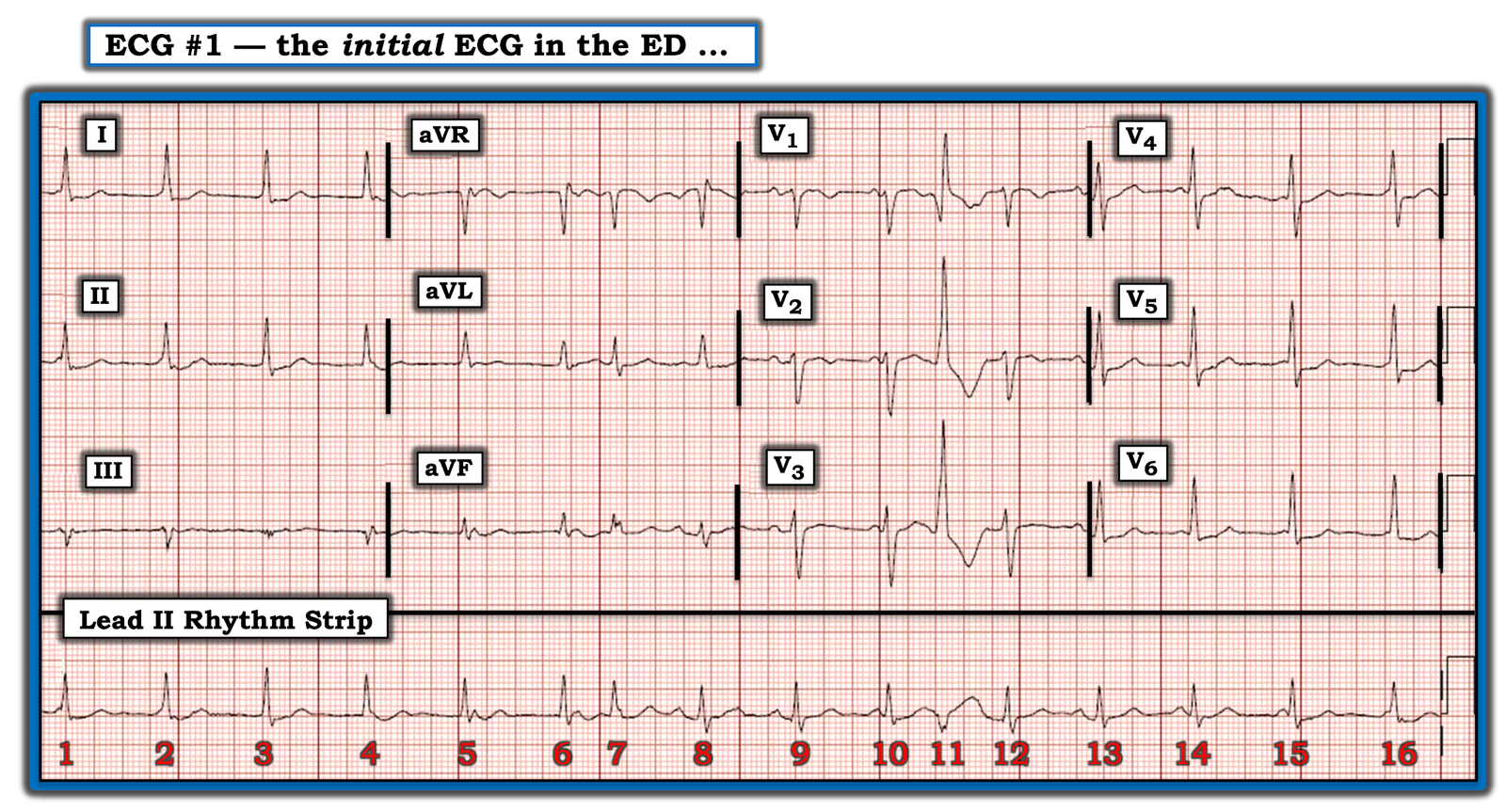
My Comment on today’s case is limited to potential assistance from use of lead aVL when assessing the initial ECG for the likely “culprit artery”:
- Unlike previous doctrine — ST elevation in lead aVL provides insight not only to the likelihood of high lateral infarction — but also to location of acute occlusion in a given portion of the anterior wall (AHA/ACCF/HRS Recs: 53 [11] 2009).
Birnbaum et al (Am Heart J 131:38, 1996) — studied the predictive value of ST elevation in lead aVL for this purpose. I summarized the conclusions by Birnbaum et al in My Comment at the bottom of the page in the February 4, 2020 post in Dr. Smith’s ECG Blog. For clarity — I’ve reproduced the Figure I used in that post below in Figure-1.
- The Figure speaks for itself regarding use of ST elevation in lead aVL for predicting the IRA.
- NOTE: Anterior ST elevation without ST elevation in aVL — suggests LAD occlusion after takeoff of the 1st Diagonal.
- Acute Diagonal Branch Occlusion: For an example of ST elevation in lead aVL (and also lead I), but limited to lead V2 in the anterior leads (ie, No ST elevation in either lead V1 or leads V3,V4,V5) — SEE this case contributed by Dr. Theodorou to the ECG Guru from 9/21/2013.
 |
| Figure-1: Clues to the “culprit artery” provided by lead aVL in acute OMI (See text). |
Regarding Today’s Case: Not every patient “reads the textbook”. There are many reasons why prediction of the “culprit artery” from the initial ECG is an imperfect art.
- What the “initial” ECG looks like will depend on when this tracing is obtained with respect to the onset of symptoms (and the onset of acute occlusion).
- Acute occlusion may be an abrupt or more gradual process — often punctuated by periods of spontaneous reopening, that may be followed again by reocclusion. This less-than-uniform process may alter ECG appearance.
- There may be variations in anatomy and/or variations resulting from development of collateral flow.
- There may be multivessel involvement.
- Other reasons.
I thought Today’s Case was especially interesting because of excellent points made by Dr. Smith in his above discussion. Some particular points to consider include:
- The degree of ST elevation in the inferior leads of today’s case favors acute RCA occlusion. This is especially true because the relative amount of ST elevation in lead III is greater than in lead II. In contrast — with LCx (Left Circumflex) occlusion — the relative amount of ST elevation in lead II tends to be more than in lead III. With acute LAD occlusion + “Wraparound” — acute inferior involvement is less likely to produce as much ST elevation as we see in today’s case in the inferior leads (especially as much as we see here in lead III).
- IF the “culprit artery” is the RCA — then the ECG finding of marked ST elevation in lead V1 tells us there is acute RV involvement and, that the occlusion must be in the proximal RCA (because the proximal RCA supplies the right ventricle).
- In favor of acute proximal LAD occlusion — is the finding in today’s case that ST elevation begins early (ie, in lead V1) — and, is present to some extent across all 6 precordial leads (with marked ST elevation in leads V1-thru-V4). When ST elevation in lead V1 is the result of acute RV involvement — ST elevation to the degree we see in today’s case is unlikely to extend so far across the left precordium.
- Finally, as per Figure-1 — the lack of any ST elevation in lead aVL favors RCA rather than LAD occlusion. To the contrary — there is marked reciprocal (mirror-image) ST depression in lead aVL with respect to the ST elevation seen in lead III. Given how early ST elevation begins in the chest leads (being marked already in lead V1 — which would suggest a proximal occlusion) — if not ST elevation, I would have at least expected some flattening of the ST segment in lead aVL if the occlusion was in the LAD (as might be seen if there was “opposition” of forces from proximal LAD occlusion with wraparound — that also caused inferior involvement).
BOTTOM Line: There are ECG findings in the initial tracing that favor both acute proximal RCA and acute proximal LAD occlusion. As a result — definitive determination can not confidently be made on the basis of the initial 12-lead.
- As per Dr. Smith — either right-sided leads and/or bedside Echo could very quickly settle the issue. In today’s case, acute cath confirmed the Echo finding of acute RCA occlusion.
- That said — Before reading what happened, I favored acute RCA occlusion because of the marked amount of ST elevation in the inferior leads with marked reciprocal ST depression (not ST elevation) in lead aVL.
- The lesson for me is HOW marked and how extensive precordial lead ST elevation can be on occasion with acute RV involvement and no LAD occlusion.
Our THANKS to Dr. Smith for presenting today’s insightful case.
![]()