The time window for therapy with thrombolytics is up to 12 hours after the onset of chest pain, based on many studies done in the thrombolytic era. However, this data comes from studies which took no account of acuteness features on the ECG.
ECGs with large upright T-waves are hyperacute, and indicate a very early MI and lots of viable myocardium.
No matter how long the duration of chest pain, patients with an ECG with high acuteness [Proportionally large T-wave, large amount of ST elevation, persistence of R-waves (R-, QR-, qR-)] indicate that the MI is not subacute, but acute, and thrombolytics may be given.
Subacute MI that is beyond the thrombolytic window, and consistent with a true duration of 12 hours or more, has smaller T-waves (both less tall and less bulky), often some T-wave inversion, QS-waves, ST elevation that is not very high.
Here is subacute STEMI:
Subacute STEMI. Should the patient go for emergent PCI, or can he wait until the next day?
Case:
A 60-something woman called 911 after 15 hours of chest pain. The pain was a 7/10 burning pain “above” her chest, non-radiating, not related to exertion, constant, and worsening all day. She called 911 because the pain was worsening.
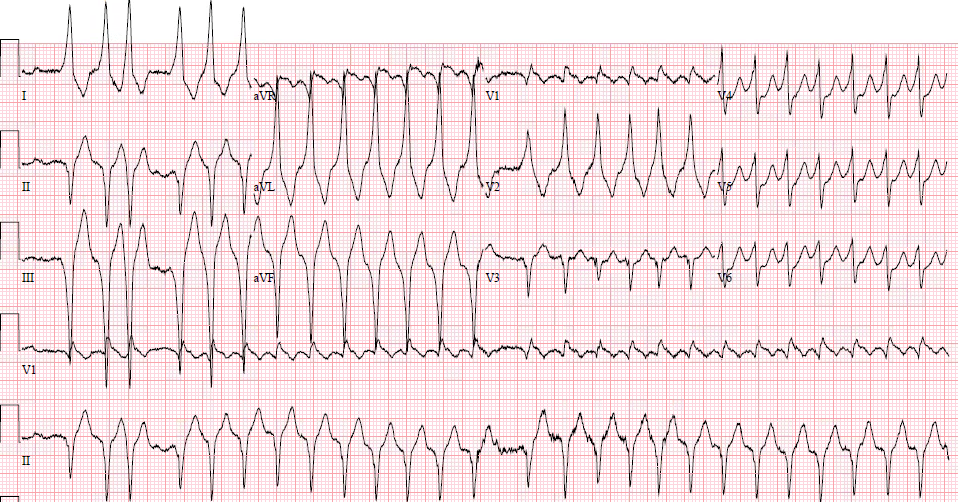
Medics recorded this ECG:
 |
|
|
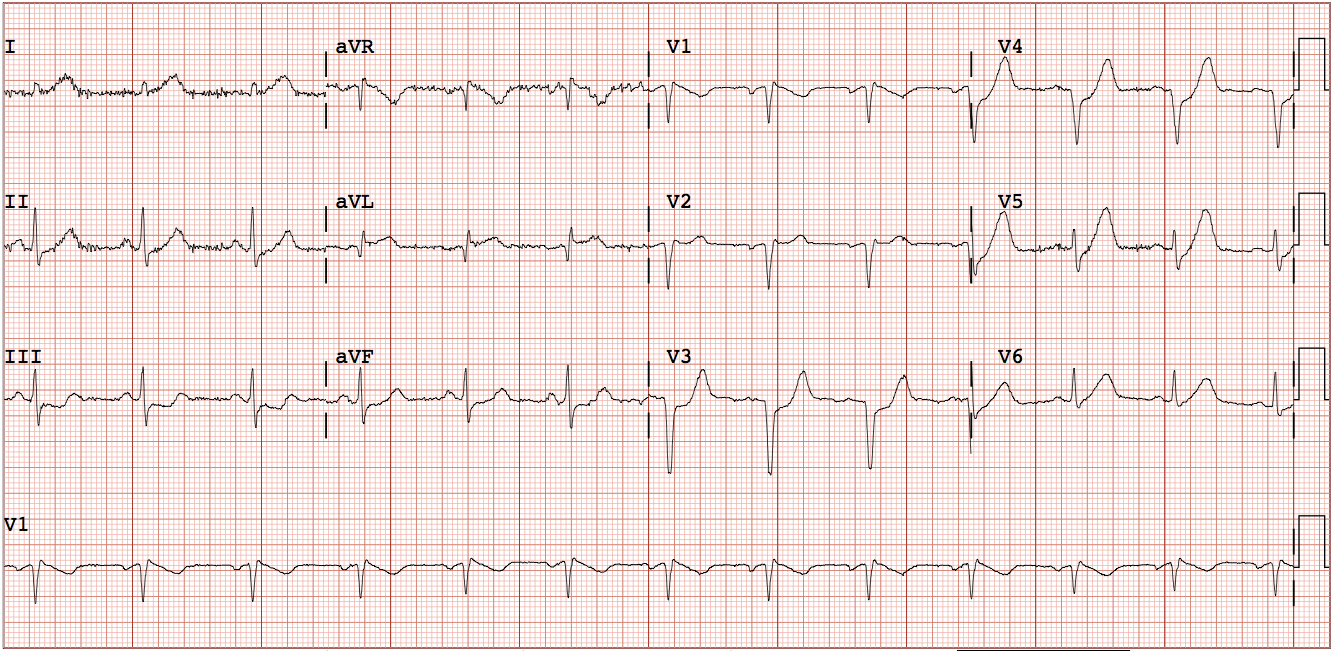
This ECG was recorded in the ED 23 minutes later:
 |
| The findings are much less obvious. There must have been some reperfusion. In fact, many might interpret this a normal or at least non-ischemic ECG (even though it is not) If you use the formulas, with QTc = 408 R-wave amplitude V4 = 7.0 ST elevation at 60 ms after the J-wave = 2.0 QRS amplitude in V2 = 6.5 3-variable formula: = 24.18 (greater than 23.4 is positive) |
If no PCI is available, and there are no absolute contraindications, then thrombolytics are indicated!!
The patient went immediately to the cath lab and had a proximal LAD occlusion.
The initial troponin I was 0.012 ng/mL (negative). In other words, this patient had unstable angina for 15 hours.
Given the ED ECG and the troponin, it is obvious that the patient’s artery is opening and closing enough to prevent any infarction, only (reversible) ischemia.
The troponin peaked at a low peak value of 2.0 ng/mL.
What if the patient had presented 13 hours previously, after only 2 hours of chest burning?
Imagine if she had come to the ED with chest pain of 1 hour duration. Her 0, 2, 4, and 6 hour troponins would have all been negative. Without a positive risk stratification score, she might have been sent home. Of course we do not know what the ECG would have shown, and it very likely would have shown at least subtle signs of LAD ischemia.
If her ECG had been normal, then her HEART score would have been 3, and she would be eligible for discharge after 2 negative troponins.
If her ECG had been “non-ischemic,” her EDACS score would have been 10, and she would be eligible for discharge after 2 negative troponins.
We will never know what her ECG would have looked like after 2, 4, 6, 8, 10, or 12 hours of chest pain, but this shows that the ECG findings can be critical added information to the clinical presentation and serial negative troponins.
Any suspicious ECG findings in this patient who would have had serially negative troponins would have to be acted upon with at least admission for risk stratification.
As you all know, I have posted many cases of positive ECGs with negative troponins.
Unstable Angina still exists.
We don’t know what “high sensitivity” troponins would have shown, but I suspect that early on, in this case, they would not have been “positive.”
Learning Points:
1. Thrombolytics are indicated in STEMI even if there is prolonged duration (greater than 12 hours) if the ECG shows high acuteness.
2. High Acuteness is measured by large T-waves, large amount of ST elevation, and absence of QS-waves.
2. Unstable Angina still exists. If a patient has a low risk score and 2 negative troponins, they are still high risk if the ECG shows any signs of ischemia.
High sensitivity troponins
There are no studies which show safety of high sensitivity troponins without use of the ECG.
This paper shows that the ECG is essential for obtaining 100% sensitivity, even with 2 high sensitivity troponin I:
Here is a pathway just published for hs troponin T. Note that is still uses ECG and risk stratification!!
Using High-Sensitivity Cardiac Troponin T for Acute Cardiac Care