This is another case provided by Mustafa Alwan, an internist from Jordan, on Facebook EKG Club
This is a 25 year old male diabetic who presented with epigastric heaviness for 12 hours. The discomfort was intermittent and associated with sweating and dizziness; it was increased increased by lying flat and relieved when sitting up.
Here is his initial ECG, with pain and diaphoresis:
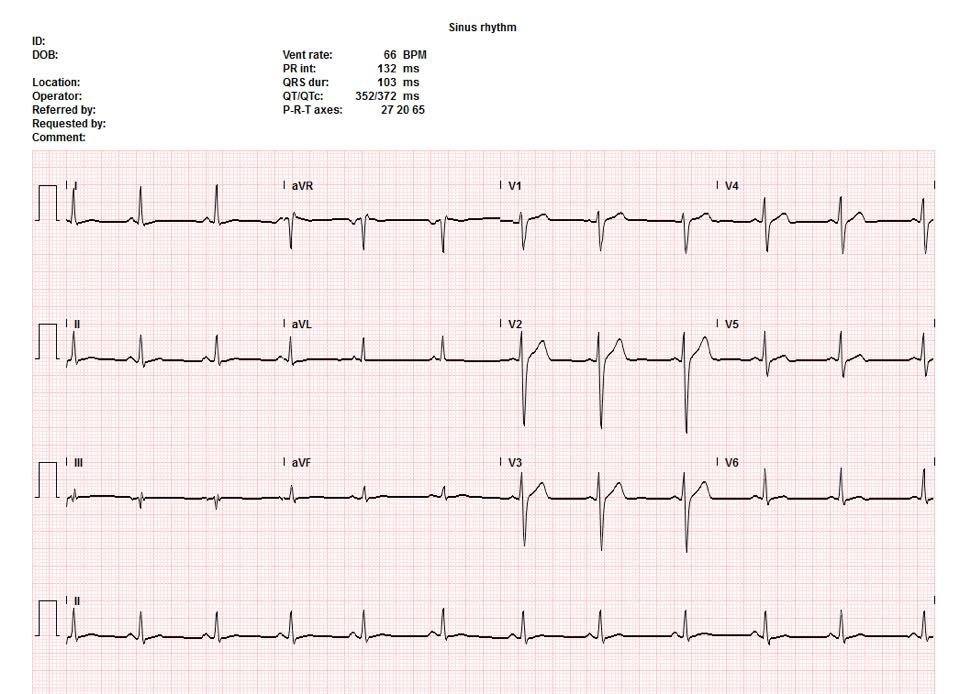 |
| It is really quite normal. When I first saw it, I did not know the patient still had pain, and I responded on FB: “This is normal. However, the sharp downturn of the T-wave in V4-V5 suggests possible development of Wellens’ waves, but is nonspecific. The T-wave flattening in limb leads is non specific.“ However, with ongoing pain, these are unlikely to be vestigial Wellens’ waves. |
He was given NTG and Morphine and pain was improved.
An interventionalist was consulted.
He performed an echocardiogram which showed no wall motion abnormality.
The first Troponin T returned at 0.017 ng/mL, slightly elevated but indeterminate.
The interventionalist diagnosed pericarditis and prescribed an NSAID.
[This ECG shows no evidence of either pericarditis or of STEMI. The diagnosis must have been based on the positional nature of the pain.]
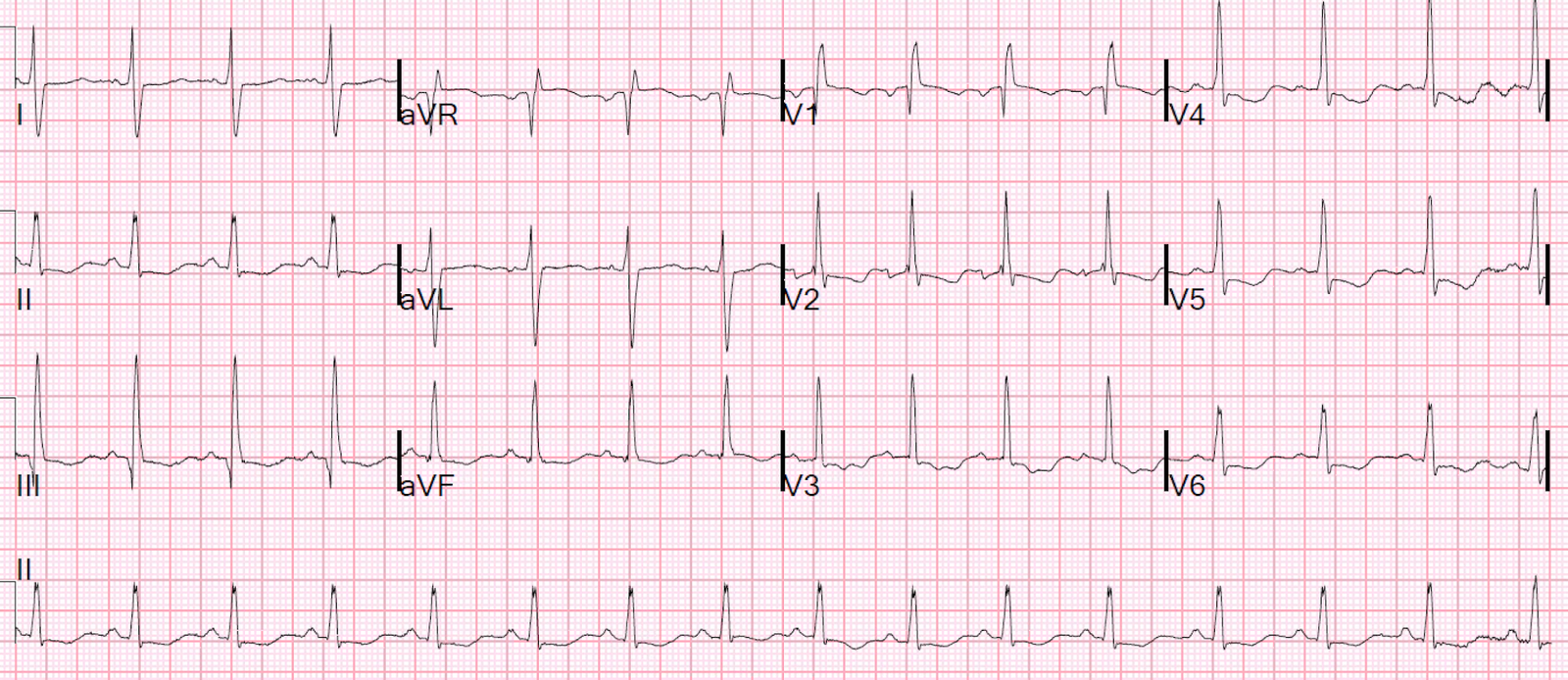
Dr. Alwan smartly recorded more ECGs. Here is the second one recorded 4 hours later:
 |
| No significant change |
6 hours after the first ECG, and 2 hours after the 2nd, a third ECG was recorded:
 |
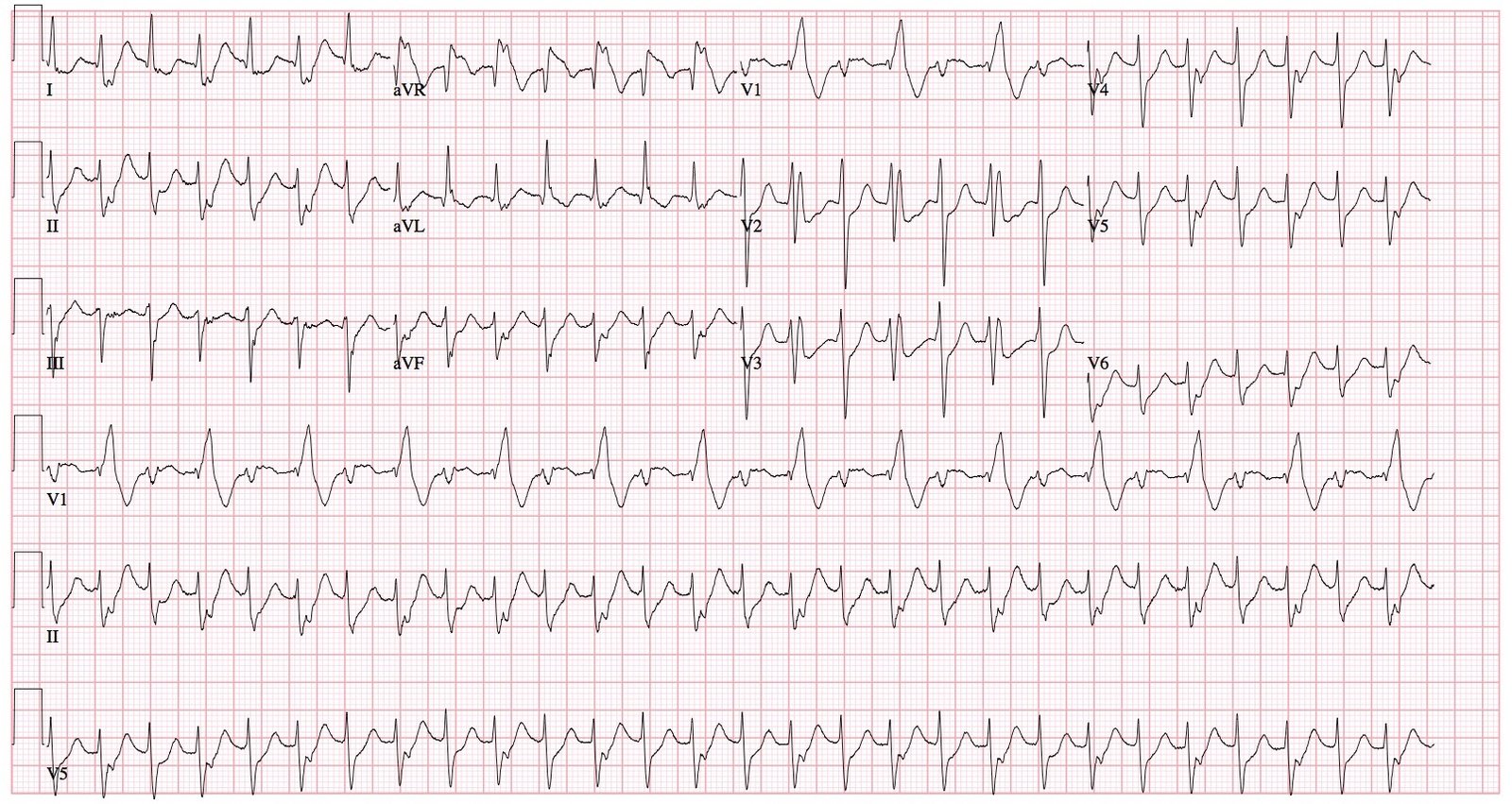
| Now there is new ST elevation, the change being diagnostic of LAD occlusion. This is not an ECG one would see with pericarditis, which manifest inferolateral ST elevation. Even if this were the first and only ECG, the differential diagnosis would be early repol vs. LAD occlusion, and the formula could be used: STE60V3 = 2.5 mm |
The patient was taken for angiogram. Here is the report:

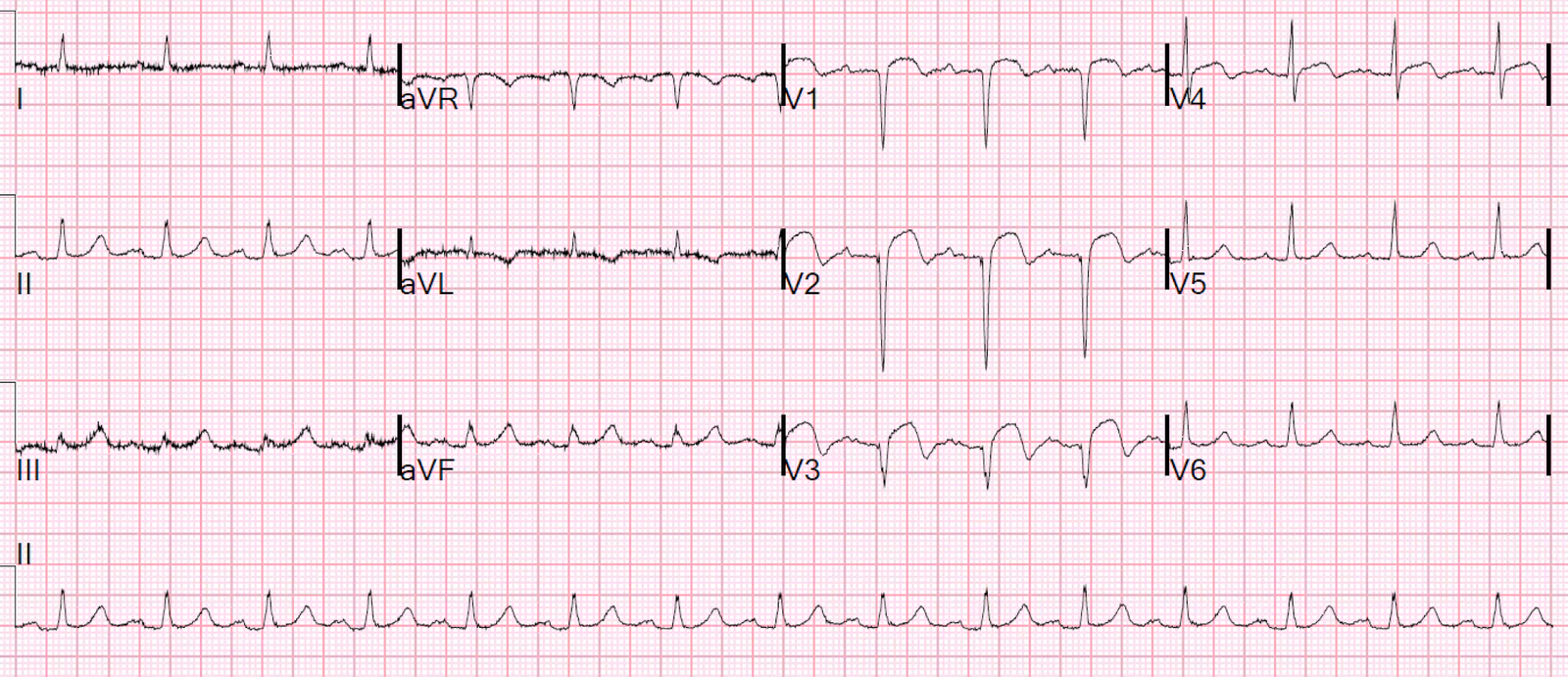
Here is the post reperfusion ECG
 |
| Typical reperfusion T-waves, identical to Wellen’s waves (Wellens’ waves represent reperfusion!) |
Learning Points:
1. Young People can have myocardial infarction
2. Though positional pain lowers the likelihood that chest pain is MI, it does not eliminate it!
3. Always get serial ECGs.
4. Pay attention to even slightly elevated troponin levels. This could have been myocarditis, but that is a diagnosis of exclusion, after a negative angiogram.