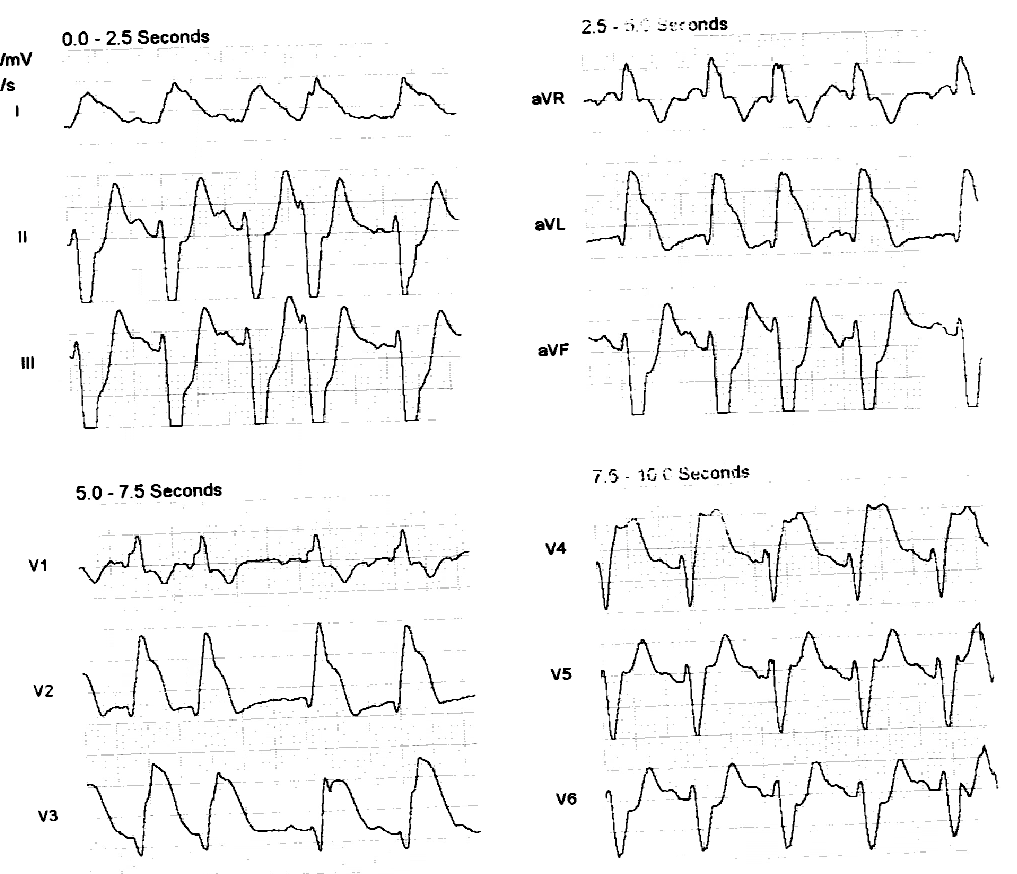
A middle-aged woman called 911 for burning chest pain and dyspnea. Here is her prehospital ECG:
 |
| There is clearly acute myocardial injury with ST elevation in high lateral leads. |
The computer did not read STEMI, but medics were very suspicious and brought the patient to the critical care area.
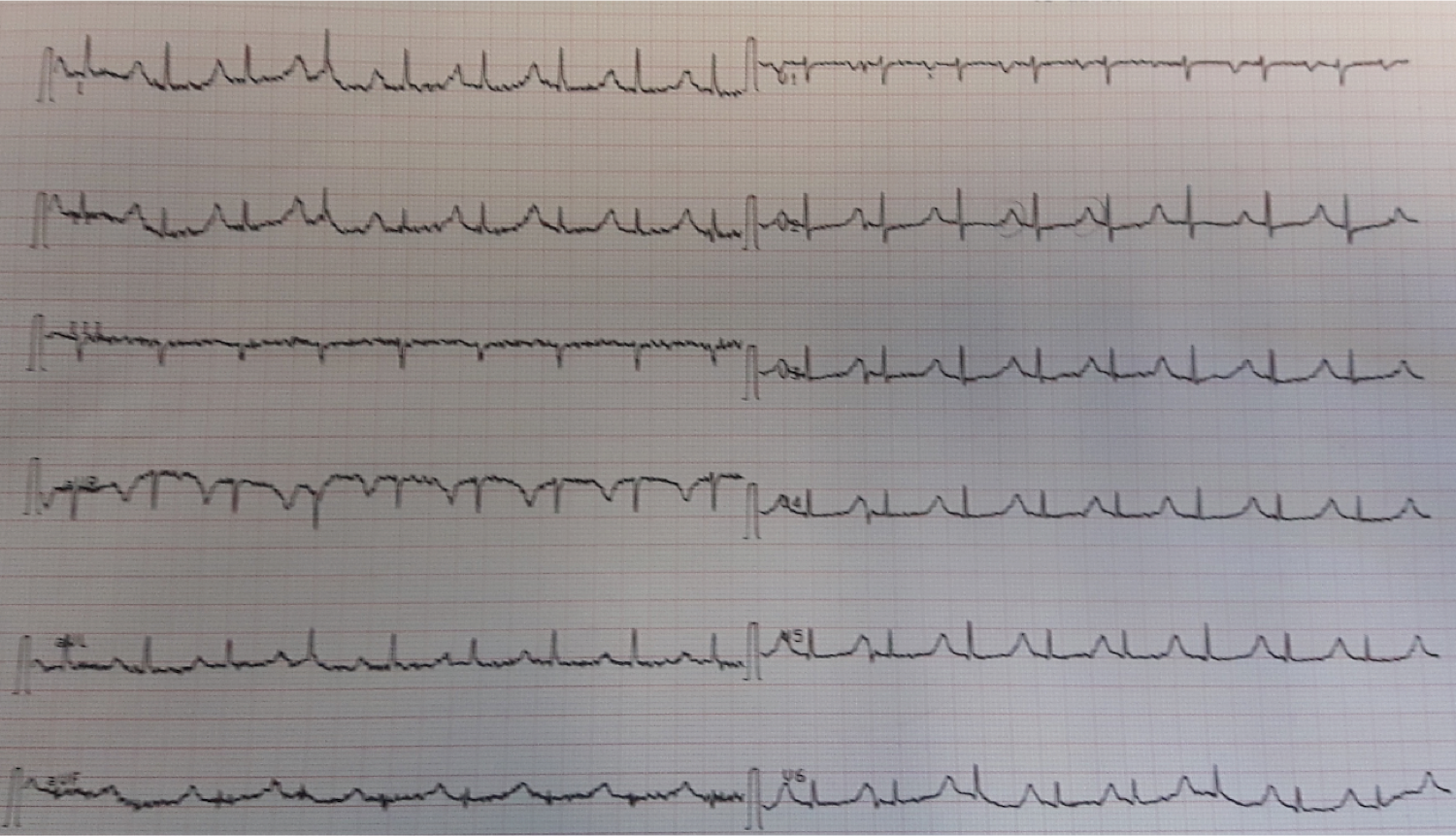
An ED ECG was immediately recorded:
 |
| There is sinus tachycardia. There is clear high lateral and posterior injury. |
The cath lab was activated.
History:
The patient states she has had 3 days of burning chest pain and SOB. She thinks she has the flu and states that she is currently pain free.
These are her first vital signs:
101/65
127
18
100.3
A bedside cardiac ultrasound was done:
Here is the parasternal long axis:
There is a moderate size pericardial effusion and some collapse of the RV
Here is the short axis:
Technique is not optimal, but there appears to be a lateral wall motion abnormality and poor ejection fraction.
With the prolonged pain and pericardial fluid, there was concern for subacute MI with myocardial rupture, and also for myocarditis/pericarditis.
Clinical course:
The angiogram was normal.
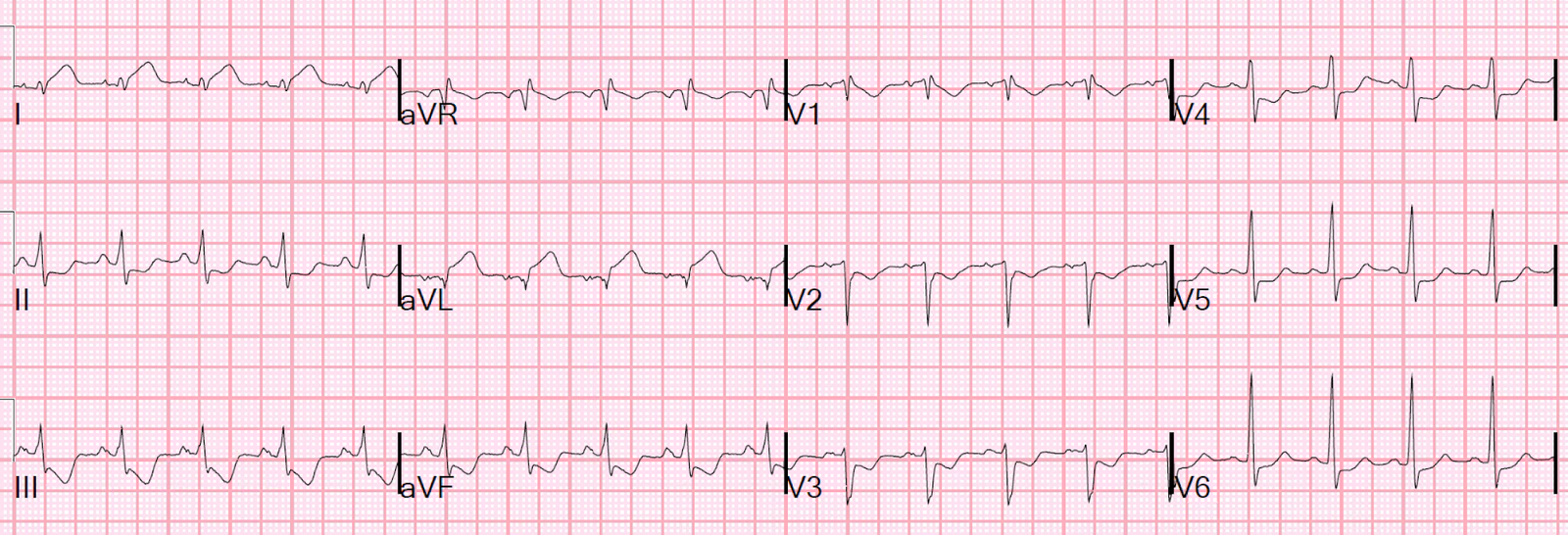
Here is the post cath ECG:
 |
| Even more ST elevation, and ST depression reciprocal to injury of the posterior wall |
A formal echo showed:
Decreased left ventricular systolic performance moderate .
Regional wall motion abnormality-lateral .
Regional wall motion abnormality-inferolateral .
Regional wall motion abnormality-anterolateral probable.
The estimated left ventricular ejection fraction is 35 %
The first troponin I returned at 33.7 ng/mL (33,700 ng/L)
3 hours: 30 ng/mL
8 hours: 32 ng/mL
10 hours: 43 ng/mL
44 hours: 16 ng/mL
ECG 2 days later:
Echo 2 days later:
Sinus tachycardia of 125-130 bpm.
Normal left ventricular size, mild hypertrophy and severe systolic dysfunction.
The estimated left ventricular ejection fraction is 25-30 % (visually estimated).
The patient became quite ill from cardiogenic shock due to myocarditis.
Learning Point
This case demonstrates that it is all but impossible to differentiate between acute MI and myocarditis.
Both may have:
1. ECG: Focal ST elevation with reciprocal ST depression
2. Echo: Focal wall motion abnormality
3. Very high troponin
4. Pericardial fluid (common in myo-pericarditis), possible in subacute MI if there is either postinfarction pericarditis or myocardial rupture
With the presence of fever, one might suspect myocarditis, but it would be dangerous to make any conclusions before studying the coronaries.