This was contributed by Brooks Walsh, who has contributed many interesting cases and articles to this blog. I edited and added comments, of course.
The Case
A
30 year-old man presented to the ED with chest pain. It had started 2
days ago, was constant, and radiated down his left arm. It was only
mild, but he also endorsed mild dyspnea. He had no medical problems. He
denied cocaine or other stimulants. Vital signs were normal, and the
exam was notable only for a thin body habitus.
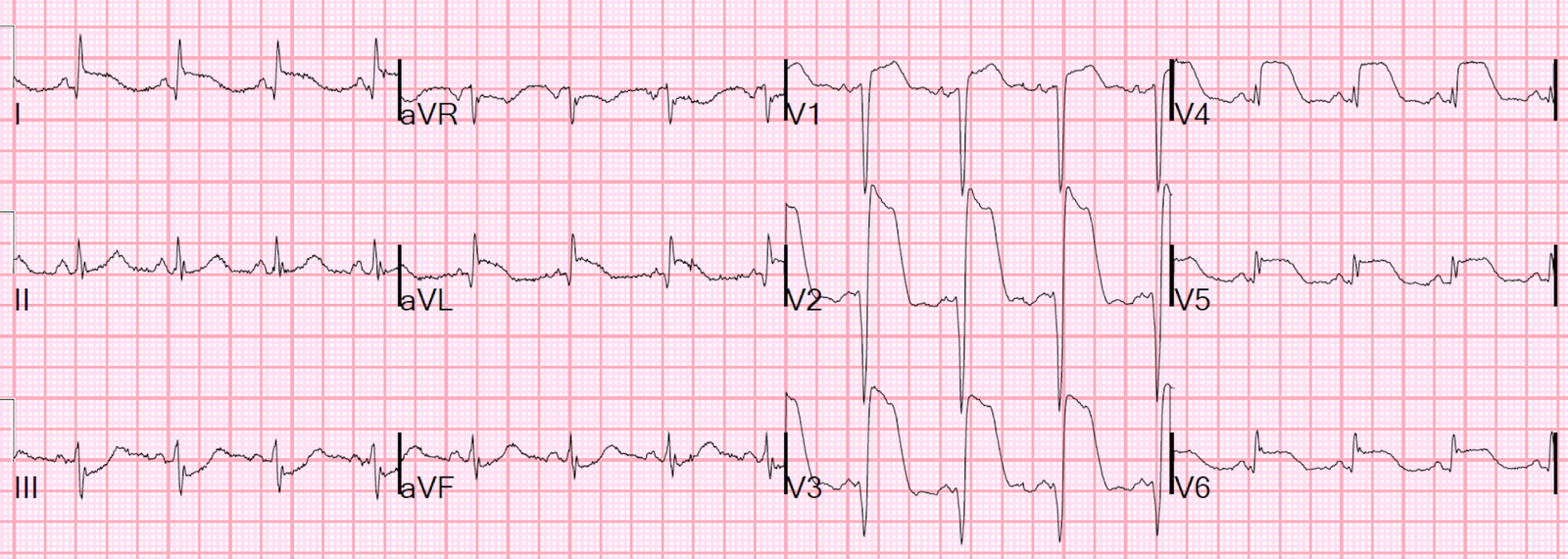
Here is his ED ECG:
 |
| There is significant anterior ST segment elevation (STE). However, the tall R waves and T waves suggest early repolarization, as do the upward-convex ST segments, and the lack of reciprocal depression. |
So is this just Early Repol?
A calculation of the “subtle anterior STEMI score” returns a value of 23.4 (using QTc = 399 ms, R in V4 = 15 mm, and STE V3 = 4 mm). This borderline score suggests this is an ACO.
However, this score should not be used, however, since lead V3 shows clear terminal QRS distortion (TQRSD), was is an exclusion for using the score.
 |
|
|
Terminal QRS distortion
When TQRSD is found with an obvious acute coronary occlusion (ACO), aka STEMI, it portends a worse response to reperfusion, and higher mortality. It is defined as:
-
In an inferior ACO, a J-point that is > 60% of the R wave height.
-
In an anterior ACO, loss of the S wave in V2 or V3.
It can also be used to identify an ACO when a subtle anterior occlusion is suspected. In this case, however, extensive clinical experience suggests that such a TQRSD will NOT show a slurred J-point (aka J wave). TQRSD was an exclusion when the score was developed and validated.
Of 355 Consecutive cases of LAD Occlusion studied, 212 were excluded as “Obvious” and 40 of these 220 had as the primary reason for exclusion “terminal QRS distortion,” defined at absence of BOTH an S-wave and a J-wave in EITHER of leads V2 or V3. Of 171 cases of proven early repol (patients who presented to the ED, had all negative troponins, had at least 1 mm of ST elevation in V2 and V3, and whose ECGs were coded as “early repolarization” by the reading cardiologist), zero had QRS distortion.
The cath lab was activated and the patient was taken for angiography
Angiography showed no significant coronary disease. The troponins, however,
initially
returned at almost 7 ng/ml [normal, less than 0.034 ng/mL (99% reference)], and peaked at 13 ng/ml.
Cardiac MRI showed, however, “patchy mid myocardial enhancement …
consistent with myocarditis.”
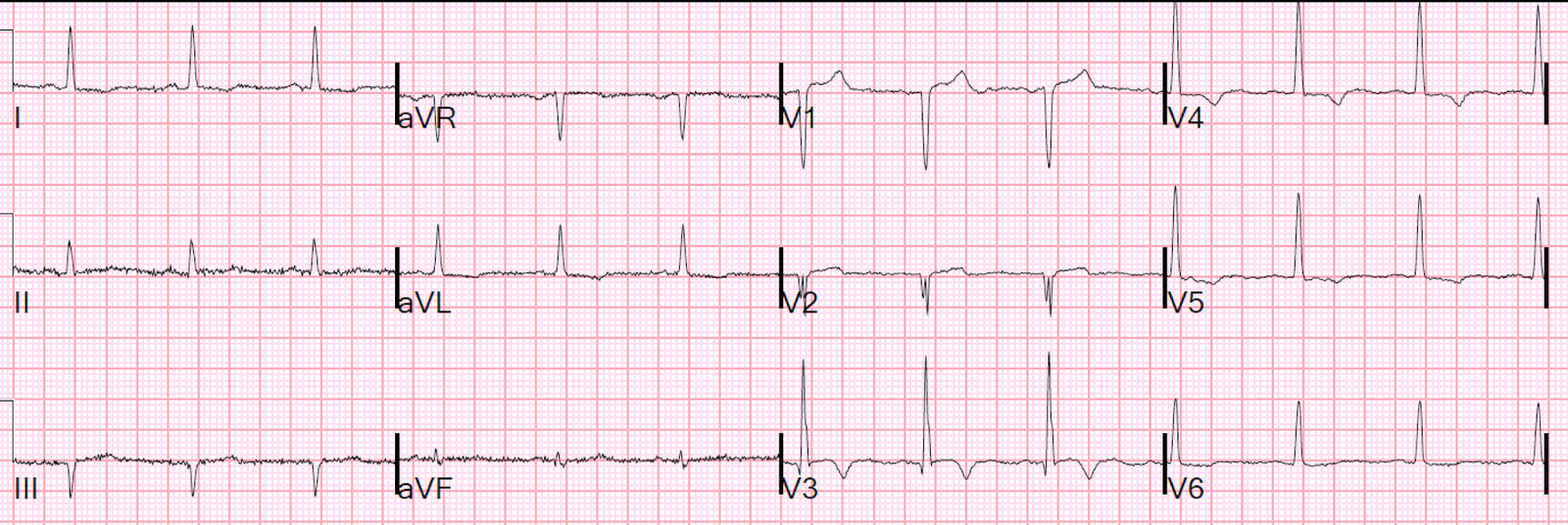
An ECG the next day:
 |
| The STE in leads V2 and V3 has decreased, as have the dramatic T waves in those leads. There are also new T wave inversions in many leads. This could be attributable to myocarditis. |
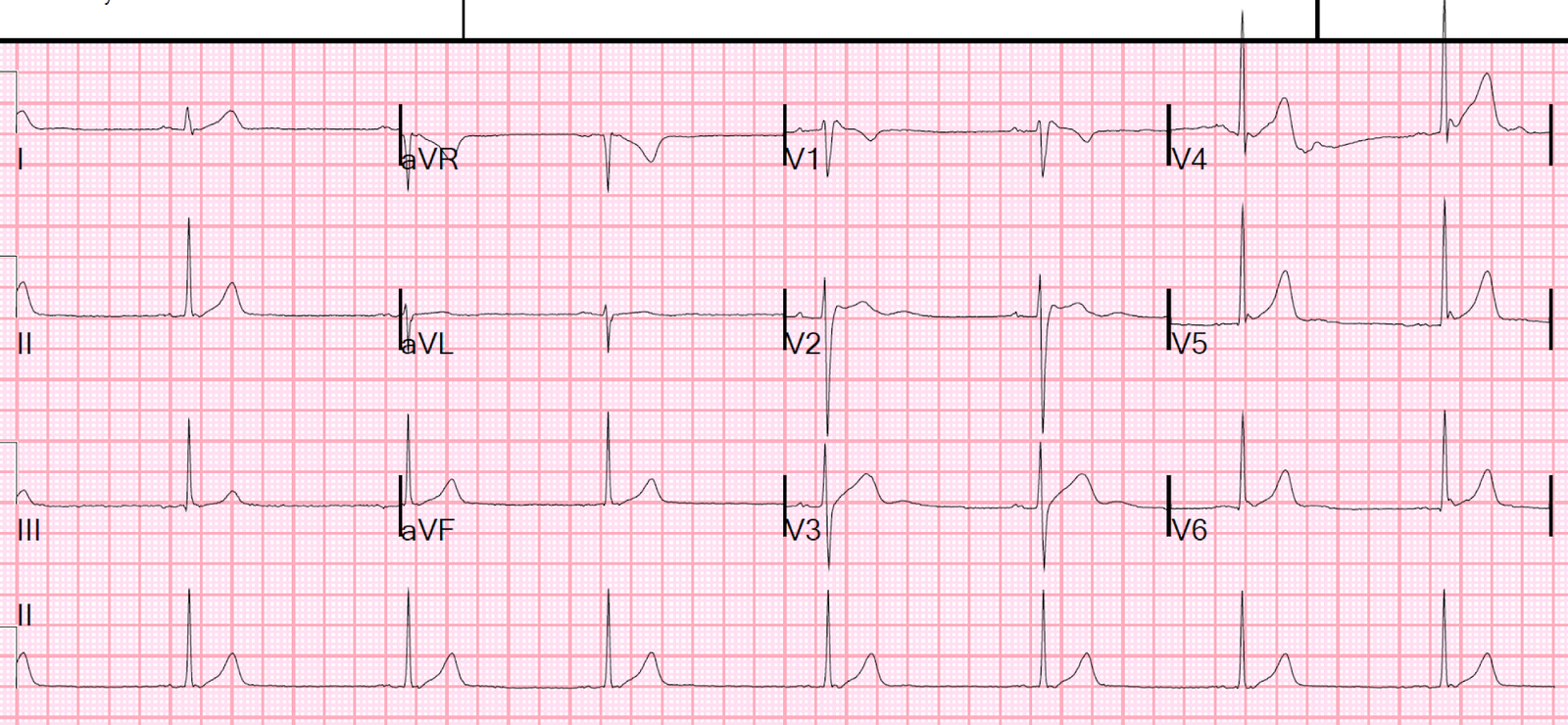
Note that V3 now DOES have a J wave, with an elevated J-point with a “fishhook” QRS/ST morphology:
![]()
False-positive TQRSD?
This is NOT a false positive, as TQRSD is used to differentiate early repolarization from pathologic ST elevation. In this case, it certainly detected pathologic ST elevation and correctly ruled out early repolarization as the cause of ST elevation.
Learning Points
1. Although TQRSD is not seen in early repol, it does NOT differentiate between myocarditis and STEMI.
2. Other cases of myocarditis show how it is often impossible to differentiate from myocardial infarction without an angiogram and MRI. Both have positive troponins, wall motion abnormalities, and even reciprocal ST depression