This patient presented with cardiac arrest:
 |
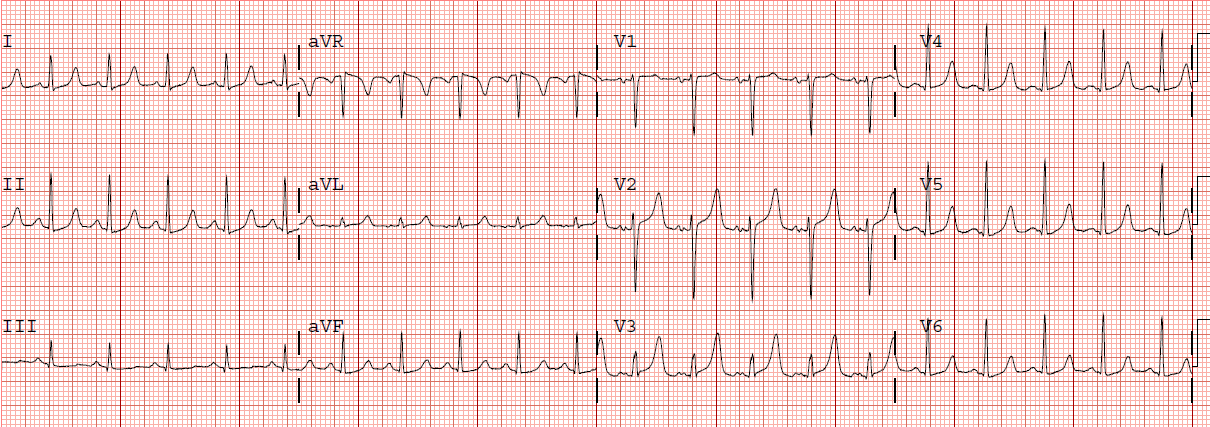
| There is RBBB and ischemic ST elevation in V1-V3. There is ST elevation in aVL and ST depression in III. This is all consistent with a proximal LAD occlusion. Should the patient go to the cath lab? |
The answer depends on the clinical situation, of course!
This is a young patient who had pulseless, non-shockable cardiac arrest. He was found with heroin paraphernalia. He was resuscitated with ventilation and epinephrine.
So this is a type 2 MI with ST Elevation. Not all ischemic ST elevation is due to plaque rupture. Only if it is a result of plaque rupture is there an indication for emergent coronary angiogram.
The etiology of cardiac arrest was respiratory, with hypoxia as the etiology. The ischemia on the ECG is due to a combination of hypoxia from hypoventilation and severe hypotension while in arrest. It is not due to coronary obstruction.