This case was provided by Tom Bouthillet, who is Editor-in-Chief of EMS 12-Lead and Chief Content Architect of ECG Medical Training.
Case
An
elderly male with a history of an RCA and mid-LAD stent started feeling
ill with nausea and vomiting. 3 hours later he developed substernal
chest pain.
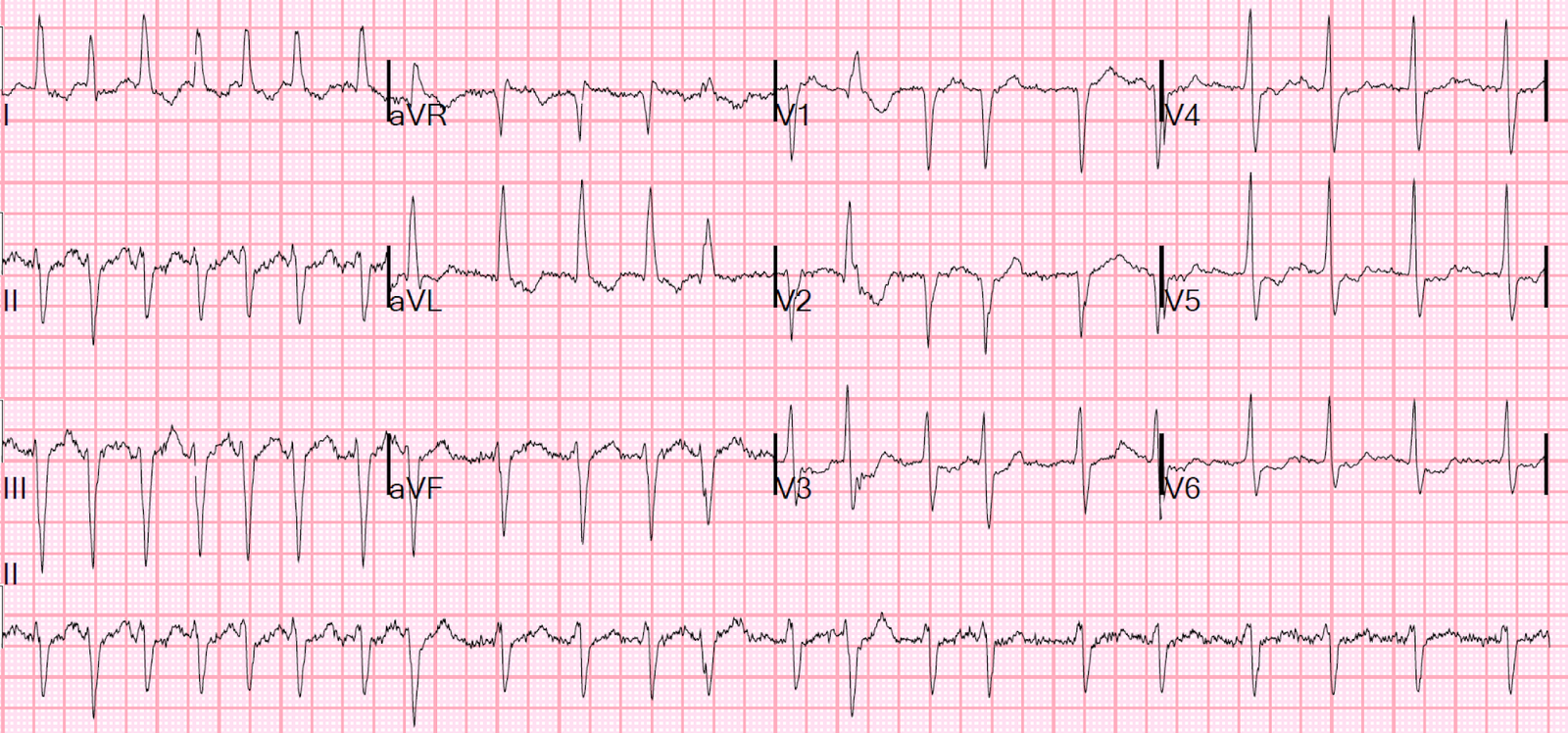
Paramedics found him with a normal exam. Pain was 5/10 without radiation or diaphoresis. This ECG was recorded:
 |
| The computer algorithm read “nonspecific”. Computerized QTc is 439 ms.
What do you think? See below. |
Sinus rhythm. There is ST elevation which is very worrisome for STEMI, especially in this high risk patient. However, there are not 2 mm of ST elevation at the J-point, relative to the PQ junction, in two consecutive right precordial leads, which is the ACC/AHA and Universal Definition of MI criteria for males over age 40 (2.5 mm are required for males under 40; 1.5 mm for women).
This ECG is very worrisome for LAD occlusion [in fact, when Tom and I (Smith) saw it, we had no doubt that it represented LAD occlusion], partly because the T-waves appear so bulky and wide. This is partly because of a slightly longer QT interval and smaller T-wave amplitude. See below:
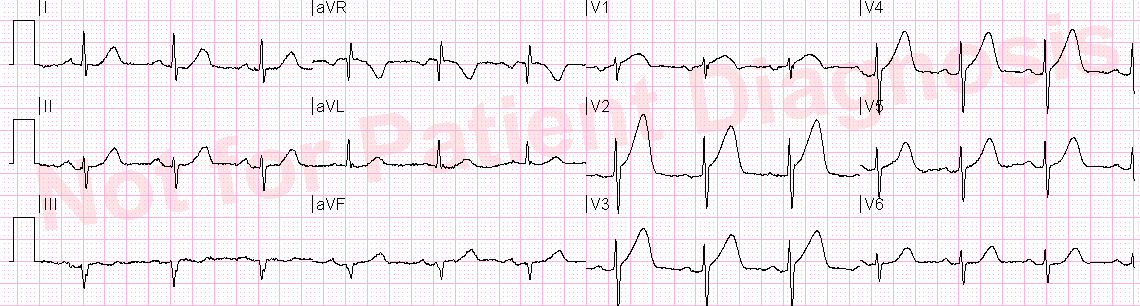
Here is V2 from a typical early repol ECG:
 |
| The STE is 4 mm at the J-point. The T-wave is 13 mm tall. |
Compare it with V2 in the above ECG.
 |
| Here there is 2.5 mm STE at the J-point. The T-wave is 10 mm tall.This looks wider and more “bulky,” don’t you think? |
What should you do when you suspect that this may be LAD occlusion?
Features to look for to differentiate subtle LAD occlusion from normal variant ST elevation in V2-V4 (“early repolorization”):
1. Early repol must have upward concavity in all of leads V2-V6 (all are concave here)
2. Early repol must not have any Q-waves in V2-V4 (there are none here)
3. There must be no “inferior” or precordial ST depression (there is none here)
4. There must be no “terminal QRS distortion” in either V2 or V3 (this means neither an S-wave that goes below the level of the PQ junction, nor a J-wave). This is explained very well here.
5. There should be no T-wave inversion in precordial leads, unless it is “Benign T-wave Inversion,” which can only be diagnosed by someone very familiar with it.
If an ECG has all these features that qualify it for early repolarization, then one should apply the early repol vs. LAD occlusion formula below.
The differential diagnosis must be only early repol vs. LAD occlusion: LVH is likely to result in a false positive.
Formula: (1.196 x STE at 60 ms after the J-point in V3 in mm) + (0.059 x computerized QTc) – (0.326 x R-wave Amplitude in V4 in mm).
STE 60 V3: ST elevation (STE) is measured at 60 milliseconds after the J-point, relative to the PQ junction, in millimeters.
A value greater than 23.4 is quite sensitive and specific for LAD occlusion. A value less than 22.0 is extremely unlikely in LAD occlusion. There is an applet on the sidebar of the blog which I have reproduced here. Just fill in the values and get the result:
A couple other findings may give a clue:
1. An upright T-wave in V1
2. Less upward concavity
In our study, we found that neither of these findings were independently associated with LAD occlusion.
The formula value is 27.2, which is clearly in the LAD occlusion range above 23.4.
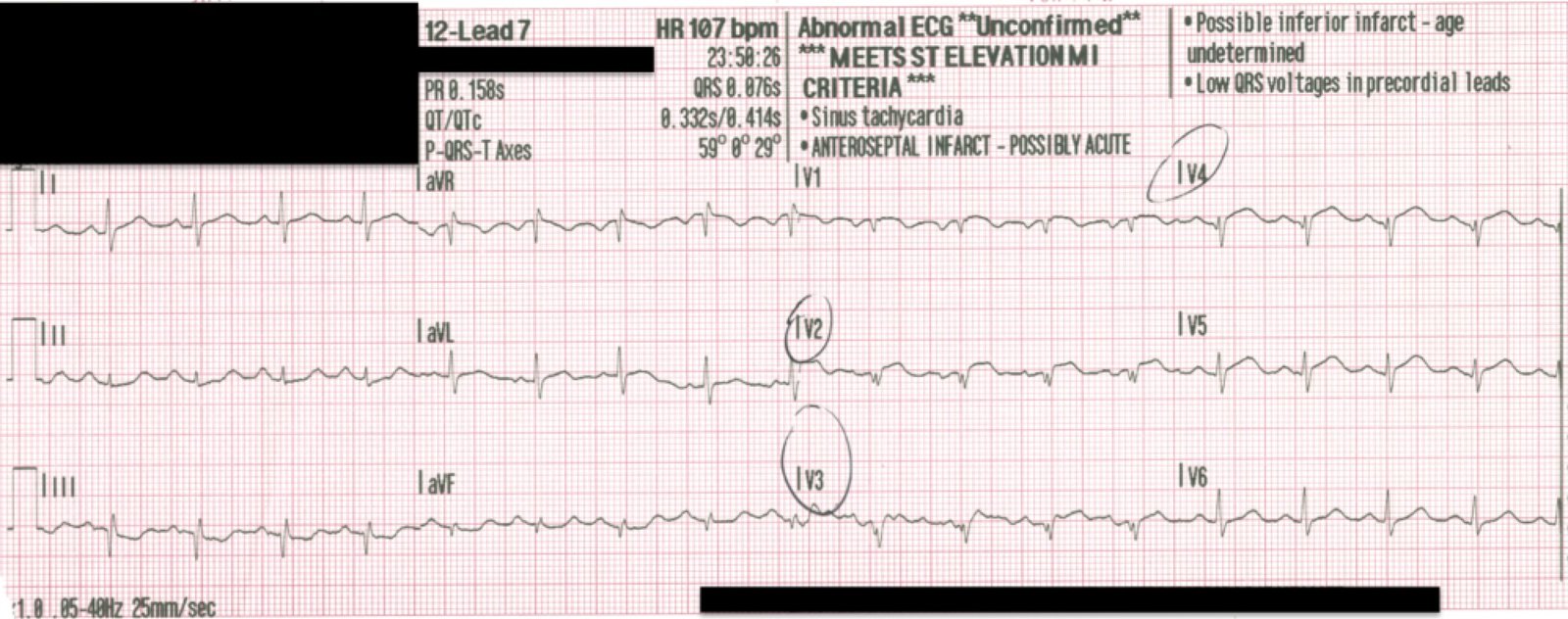
Another ECG was recorded at t = 21 minutes, when the patient was feeling slightly better:
 |
| QTc is 442. T-waves are slightly smaller, but the formula value is still over 27. |
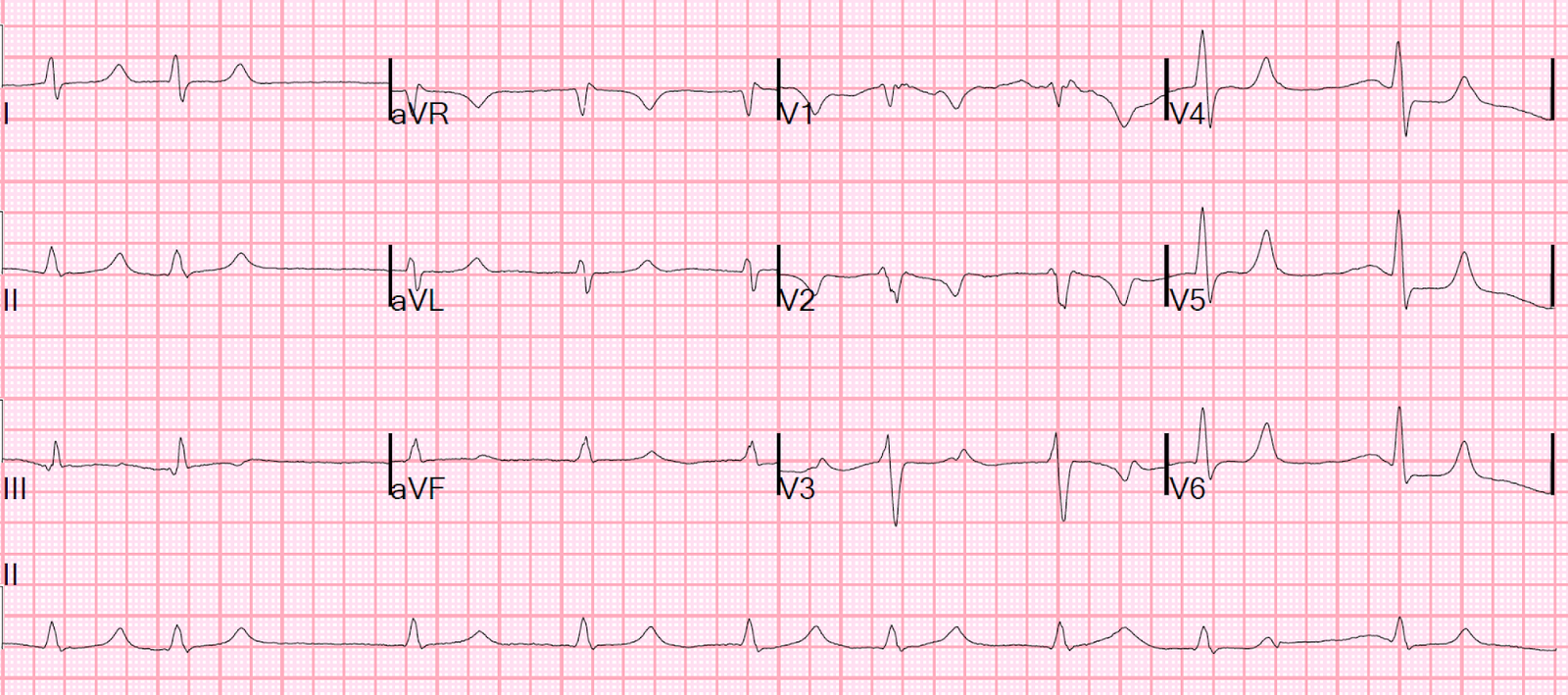
Another ECG was recorded at t = 26 minutes:
 |
| QTc is 448. No significant change. |
In
spite of these ECGs, and the high pretest probability, the patient was
only taken to the cath lab after a long delay and absence of
improvement with medical therapy.
The
exact delay is uncertain, and the exact reasoning uncertain, but
physicians still are inappropriately dependent on millimeter criteria for diagnosing STEMI
even if the diagnosis is obvious, even though these criteria are very insensitive for acute MI (less than 50%, and about 75% sensitive for occlusion
The patient was eventually taken to the cath lab and had a 100% in-stent thrombosis occlusion of the LAD.
Learning Point:
Millimeter
criteria are dangerously insensitive for acute myocardial infarction
(sensitivity 48%!), though better for acute coronary occlusion (around
70%). If you rely on them, you will miss approximately 25-30% of acute
occlusions.