A young woman presented to the ED with a complaint unrelated to any cardiac condition.
The pulse was fast. The physican noted it was irregular. The woman stated that this happens frequently for years, but she had never sought medical attention for it.
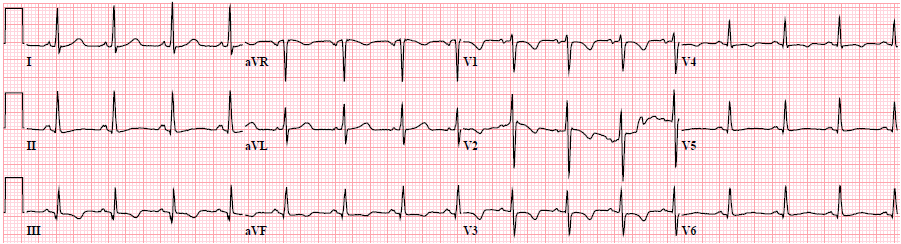
Here is the 12-lead:
 |
| The rhythm is very fast and irregularly irregular. Usually that means either atrial fibrillation or multifocal atrial tachycardia. |
—-Is it atrial fibrillation? There are clearly waves that look like P-waves, so probably not.
—-Is it MAT? No, the P-waves are unifocal (of one morphology)
—-Is it atrial flutter? They look like P-waves, not like flutter waves, which should have a continuously undulating baseline.
—-Moreover, with atrial fluter, the QRS should land on the same part of the atrial wave every time. In this tracing, the QRS sometimes lands in the middle of atrial activity, and sometimes after it.
—-Accordingly, if it is flutter, the R-R interval should be some integral multiple of the flutter interval (hence: it would be regularly irregular; here it is irregularly irregular.
—-The atrial activity looks like P-waves, not flutter or fibrillation waves.
I sent this one to K. Wang and also showed it to the members of the Facebook EKG club. The consensus opinion corresponded to K. Wang’s interpretation, which I paraphrase below:
There is an atrial tachycardia at a rate ranging from ~250 to 300 per minute with primarily 2:1 AV conduction but occasionally 3:1 or even 4:1 AV conduction which converts to NSR at the end of the 1st tracing. The baseline does not continuously undulate in any of the 12 leads, indicating there is no continuous circus movement of the electrical front, so it is not atrial flutter.
So it has to be called atrial tachycardia. EKGs at this rate are often atrial flutter, and that is why it is confusing, but in this case it is a fast atrial tachycardia. In young people, especially children but also young adults, atrial tachycardia can be very fast. It is also unusual for the atrial rate to not be consistent (here it varies, so this is unusual).
This is another important observation: It is not the P-wave directly before the QRS that is conducting, but rather the previous one.
See this ladder diagram drawn by Dr. Wang:

Acute treatment options include AV node blockade with Diltiazem or, better yet, beta blockade to attempt to slow the atrial tachycardia AND conduction through the AV node.
Metoprolol was given. Electrolytes were normal.
What else do you think is going on? Answer below.
Outcome:
The patient was found to have an undetectable TSH, and a T3 and T4 above the lab measurement capabilities. She was noted to have some thyroid “fullness,” but no proptosis. She did have thyroid antibodies (which activate the TSH receptor) and was diagnosed with Graves’ disease.
Here is a one slide summary of assessment and management of atrial tachycardia, from my lecture on SVT:
l Etiologies: Lytes, acid-base, drug toxicity, fever, hypoxia, thyroid
l Digitalis toxicity
lCorrect hypokalemia, Digibind
l Correct underlying disturbance
l Beta blocker or Ca channel blocker
l Mg (2-4 g IV)
l Adenosine occasionally terminates (only if the atrial rhythm is regular)
lSinus node re-entry or triggered activity
l Electrical treatment rarely needed
l50-100 J if unstable
l Overdrive transvenous atrial pacing
Learning Point:
Any very fast supraventricular atrial rhythm should lead to suspicion of hyperthyroidism.
Here are some rhythm strips for anyone interested: