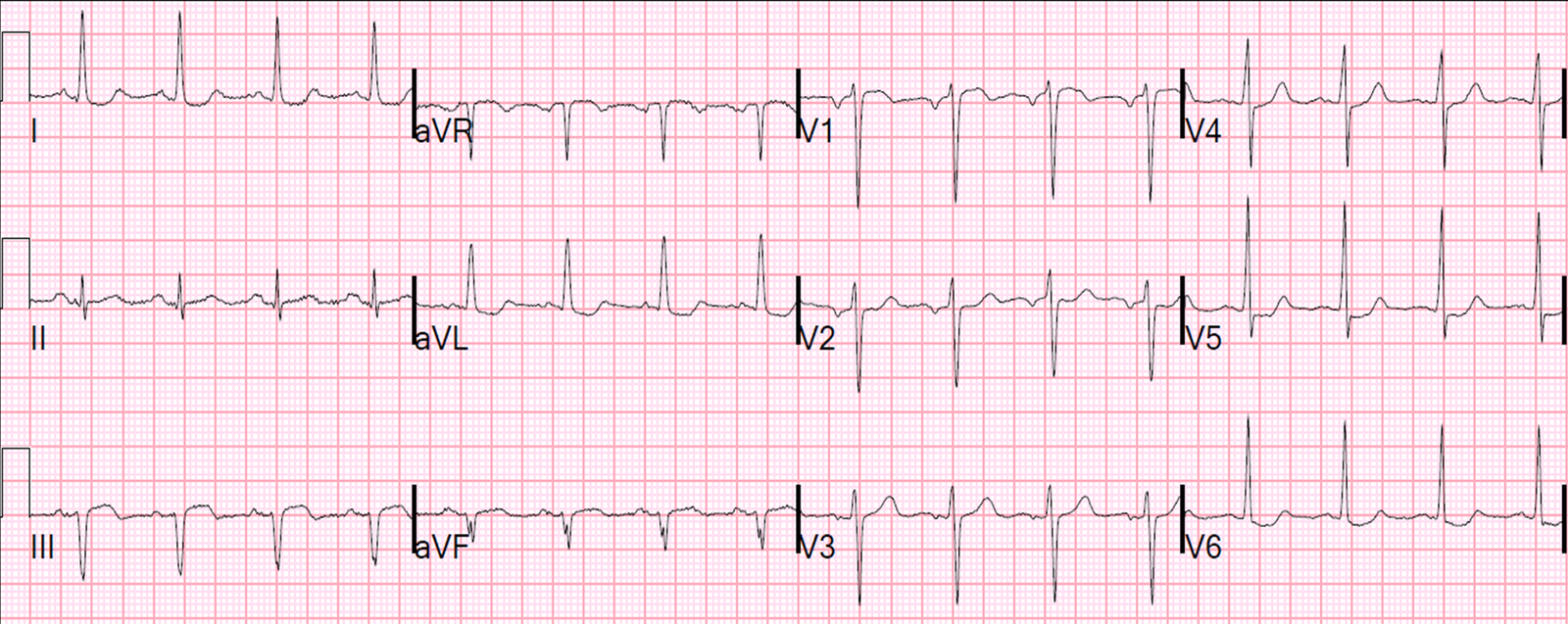
A male in his 60’s with no previous cardiac history complained of substernal chest pain intermittently for 18 hours. It has more recently become constant. He was diaphoretic. He called 911 and had this prehospital ECG recorded:
 |
| I saw this when he arrived, and was worried about the slight ST depression in V2 and the size of the T-waves in V5 and V6, as well as the minimal terminal T-wave inversion in aVL and a bit of ST depression there. |
We recorded this immediately:
 |
| The same findings are here, without any evolution. |
BP was 140/80.
His pain continued and would be relieved from 8/10 to 6/10 with sublingual nitroglycerin. We gave aspirin and clopidogrel for high suspicion of ACS.
Had I looked for it (which, foolishly, I did not), I would have found this previous ECG from 9 months prior:
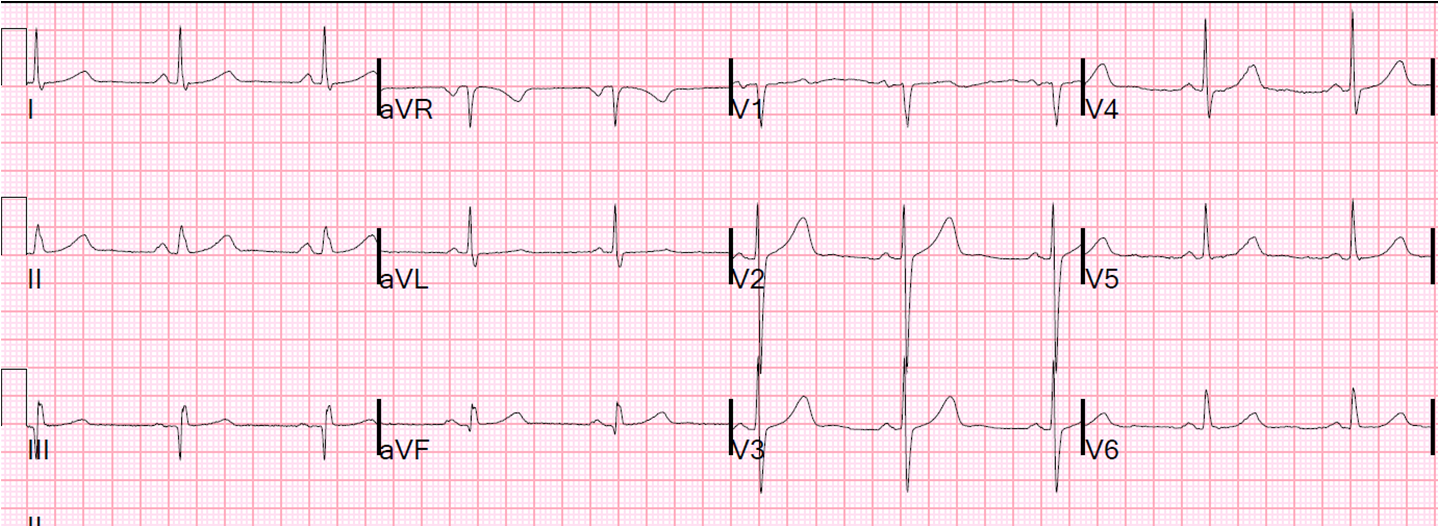 |
| There are definite changes compared to this one |
Had I seen this, I would have immediately diagnosed definite ACS and started high dose IV nitroglycerin.
As it was, we did give sublingual NTG, and sent a troponin and, while the pain continued, recorded this ECG 42 minutes later:
 |
| The T-waves in V5 and V6 have less amplitude. This caught my eye. |
Not having seen the old one yet, and seeing no diagnostic evolution, I just kept a high index of suspicion. But I was pretty sure that, with the duration of pain, that if this chest discomfort was indeed due to ACS, that the first troponin would be at least slightly elevated.
The first troponin then returned at 0.20 ng/mL (normal up to 0.030 ng/mL). The diagnosis was clear. High dose nitro was started with no relief.
We activated “Pathway B”, a system we have worked out which is intermittent between cath lab activation and no activation, and which covers patients with NonSTEMI but whom the emergency physician believes need to go to the cath lab immediately.
Patients with objective evidence of ongoing ischemia that is not relieved by anti-platelet, anti-thrombotic, and anti-ischemic therapy should go directly to the cath lab.
The cardiologist agreed, and the patient went straight up for angiogram:
 |
| The red arrow shows the very tight, hazy, acute thrombotic 95% stenosis of a very large Obtuse Marginal (this vessel is in the right position to either be a high takeoff OM, a high takeoff 1st diagonal, or a ramus intermedius, which is a vessel that is sometimes seen between the circumflex and the LAD). The black arrows point out its entire course, which now has TIMI III flow. |
Here is the post cath ECG:
 |
| The V2 ST depression is gone, and the V2 T-wave has much higher amplitude (posterior reperfusion T-wave). The T-waves in V5 and V6 are normalized. There is now T-wave inversion in aVL. There is much artifact in inferior leads. |
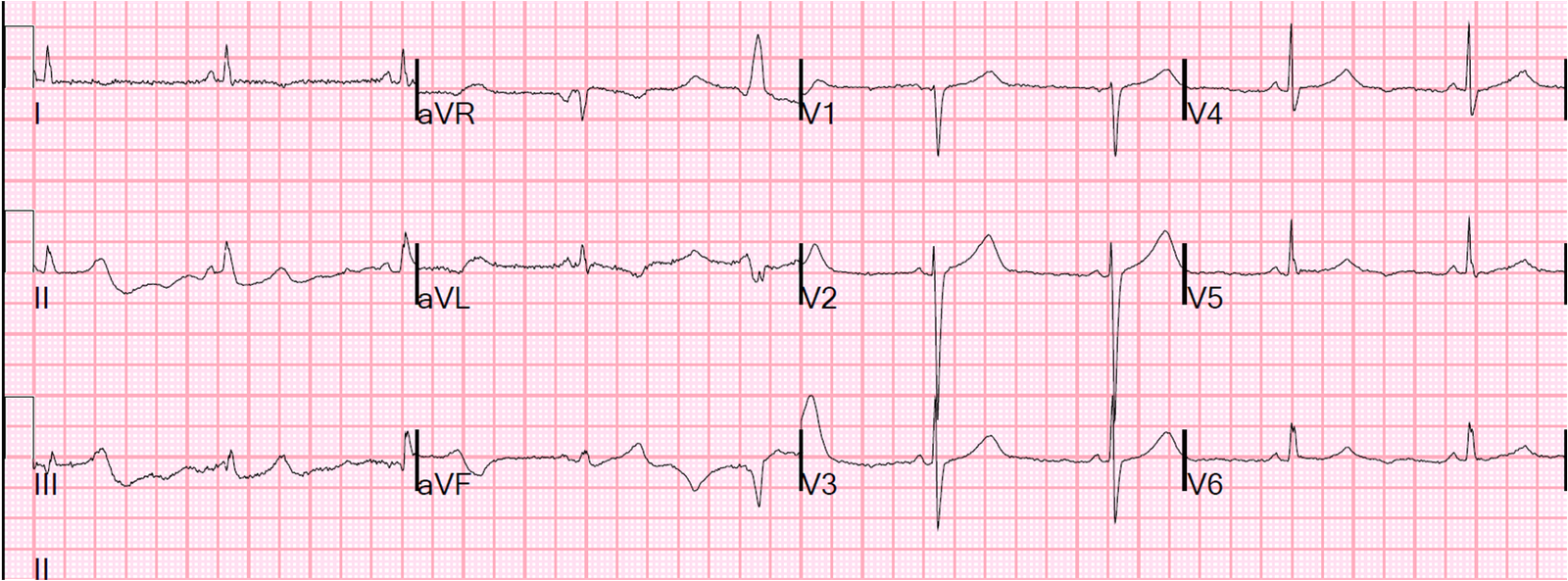
Here is the next day ECG:
 |
| There is deep T-wave inversion in I and aVL, with reciprocally large T-waves in III and aVF, and some terminal T-wave inversion in V5 and V6. |
Next day echo showed Lateral and inferolateral wall motion abnormality.
Troponin I peaked at 28 ng/mL
Learning points:
1. Aggressively investigate suspicous ECG abnormalities in the context of typical chest discomfort and unrelieved symptoms
2. Compare with the old ECG!
3. Some NonSTEMI need the cath lab now! (objective evidence of ischemia and refractory symptoms)
4. Notice that, in ACUTE posterior infarction, there is not necessarily any increase in R-wave amplitude in V1-V3. In this case, there was a decrease.