A male in his 40’s was in his usual state of health until 3 hours prior when he developed L-sided chest pressure, radiating to the neck, while walking. He called 911. His prehospital ECG is identical to the first ED ECG shown below. Based on this, the paramedics activated the cath lab, administered nitroglycerin, and the pain resolved.
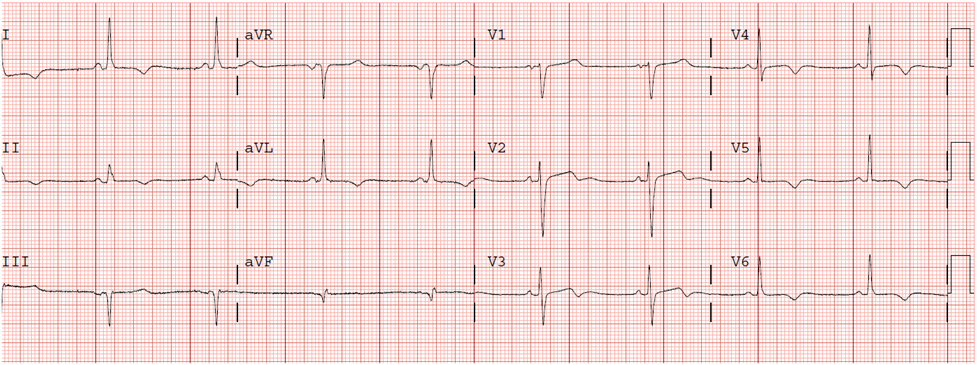
This ECG was then recorded in the ED:
 |
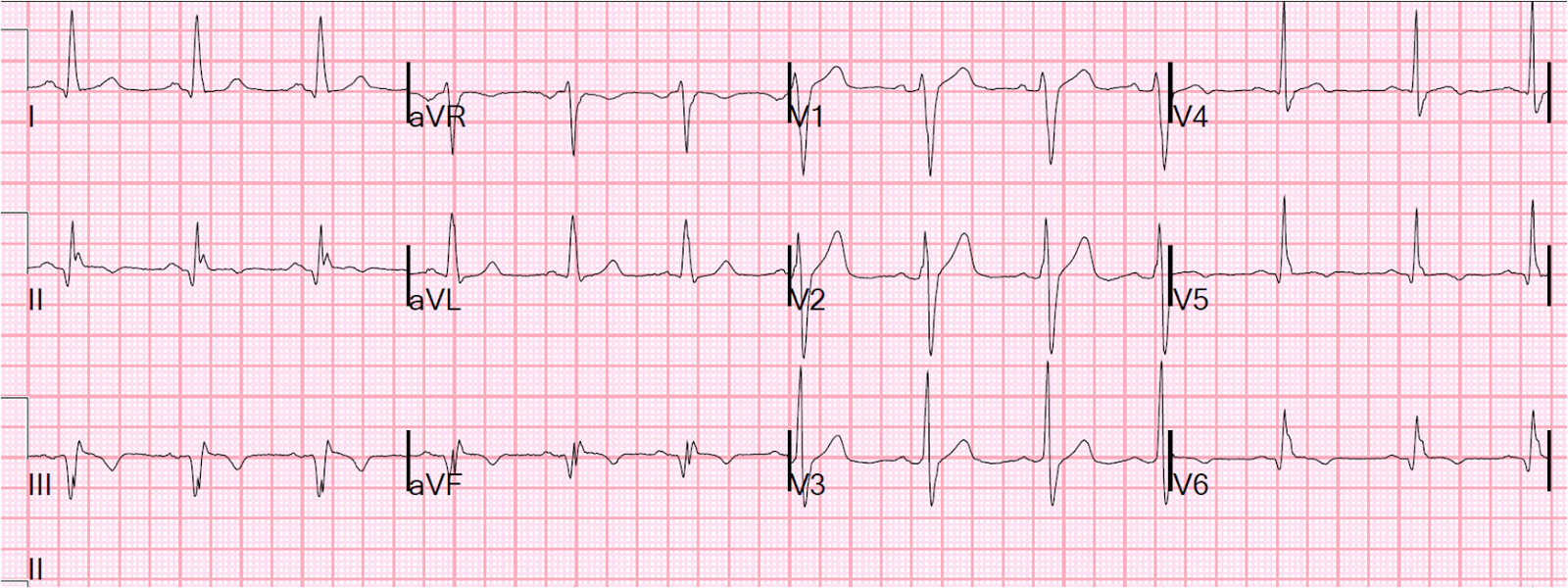
| There is at least 2 mm STE at the J-point in leads V2 and V3, but the morphology of the T-wave is typical of early repolarization (slow upstroke, fast downstroke). There is minimal ST elevation in I, aVL, V5 and V6. There are not exclusions to using the formula: no inferior ST depression, no upward convexity, no precordial T-wave inversion, no Q-waves, and no terminal QRS distortion. Thus, the Early Repolarization vs. LAD occlusion equation can be applied (see sidebar for Excel applet that can be use to make this calculation): STE60V3 is 4 mm, QTc was 416ms, and RA-V4 is 15mm. Thus, the equation value is [1.196 x STE60V3]+[0.059 x QTc]–[0.326 x RA-V4] = 23.753, which is greater than 23.4 and would indicate STEMI. The specificity of the rule is not perfect, but a value above 23.4 should at least prompt you to aggressively evaluate the patient. |
Legend
–STE60V3 = ST elevation at 60 ms after the J-point, relative to the PR segment, in lead V3
–QTc is Bazett corrected QT interval
–RA-V4 is the R-wave amplitude in lead V4
This was not recognized, and the ECG was interpreted as early repolarization. A bedside echocardiogram reportedly showed no wall motion abnormality.
A repeat ECG was recorded:
 |
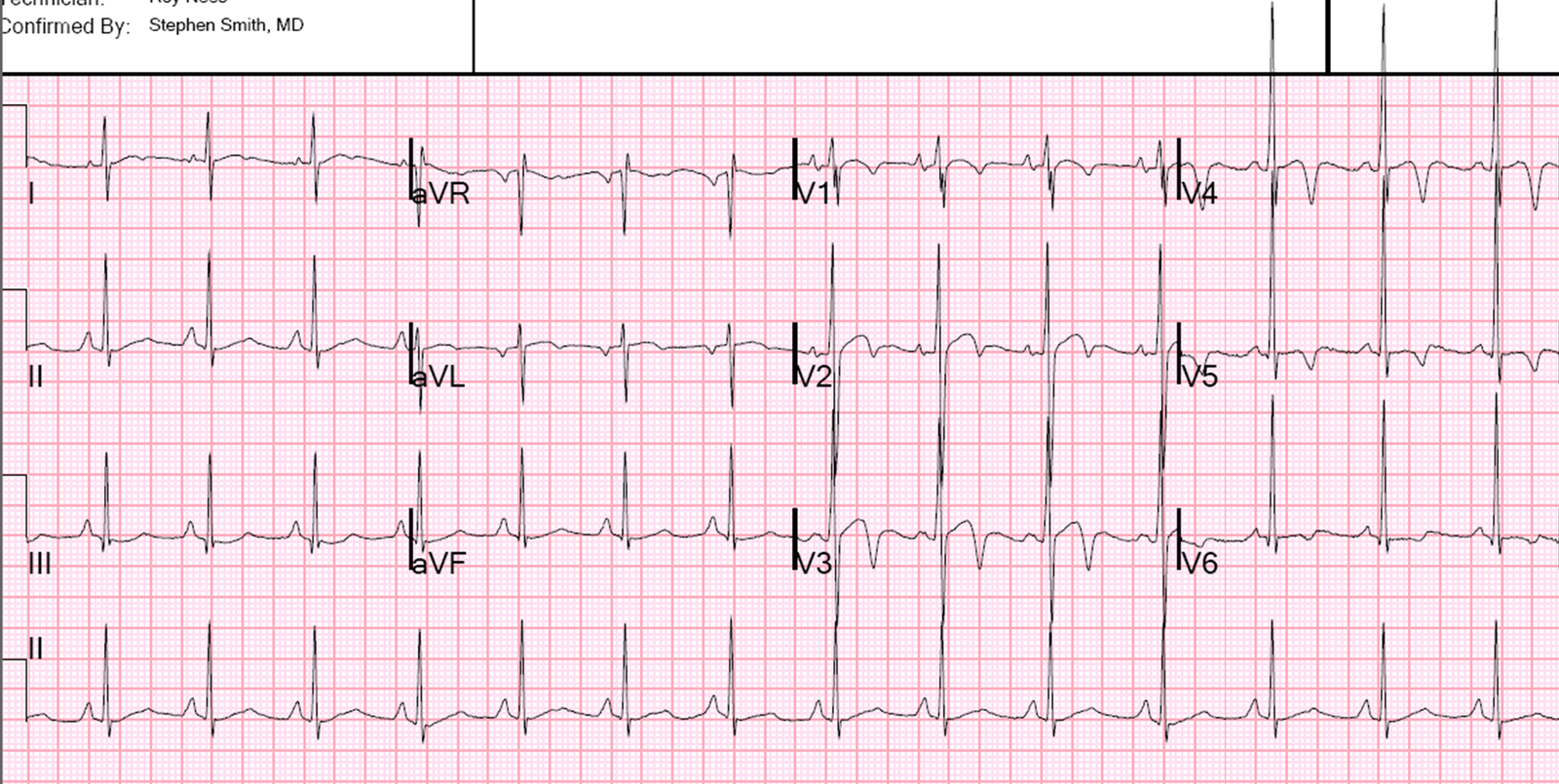
| Here, V2-V5 have less ST elevation and the T-waves are smaller. It appears normal, and different from the presenting ECG. An application of the equation has equivocal results depending on whether the STE60V3 is measured at 1.5 or 2.0 mm. |
Nevertheless, the change shows that the previous ECG was indeed due to acute coronary syndrome (ACS).
This was not seen and the cath lab was de-activated. The patient was admitted and ruled out for Acute MI with serial troponin I less than 0.04 ng/ml (using a sensitive troponin assay).
Not all ACS has a positive troponin. When negative, it is of course called “unstable angina.” Unstable angina (see more such cases here) usually presents with a normal or nonspecific ECG, or with ST depression or T-wave inversion, but it may present with transient ST-segment elevation. And, surprisingly, transient ST elevation does not always result in a positive troponin. The ischemia may resolve so quickly that there is both no wall motion abnormality and the troponin is negative!
With the advent of high sensitivity troponin in the future, perhaps such cases will become more rare. But this increased sensitivity may come at the expense of worse specificity, or more false positive troponins.
The patient was discharged, and 13 days later presented with identical chest pain, which again resolved, and had the following ECG after resolution of pain:
 |
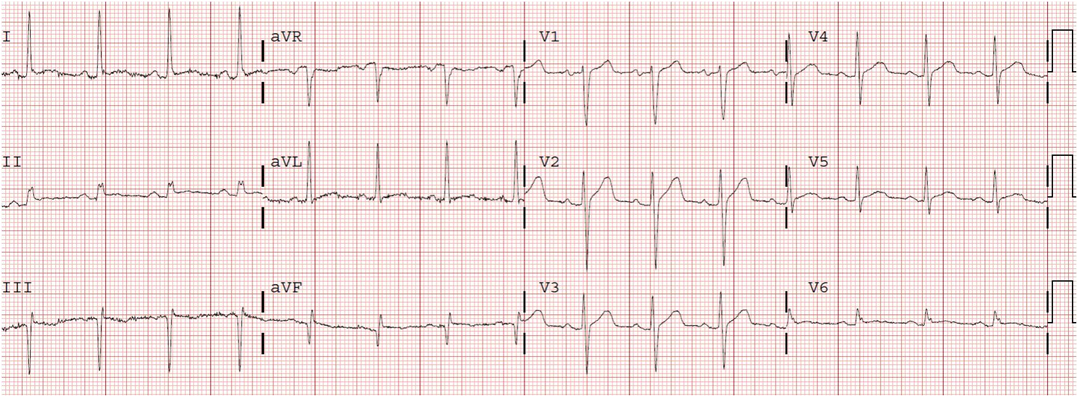
| There is new T-wave inversion in I, aVL, V4-V6. There is terminal T-wave inversion (biphasic) in V2 and V3, but complicated by the U-waves seen in these leads. This T-wave inversion represents a form of Wellens’ syndrome, indicating spontaneous reperfusion of a brief left anterior descending coronary occlusion. |
Outcome: This time, the troponin was positive [which one would expect when there is not just resolution of STE, but also T-wave inversion (Wellens’)]. The patient underwent coronary angiography, which showed severe subtotal LAD disease and 70% left main disease. He underwent coronary artery bypass surgery.
This case illustrates the importance of paying close attention to the ECG and its evolution. Using the formula may help.
Lessons:
1. Coronary occlusion may be brief, with spontaneous reperfusion.
2. Serial troponins may be negative even in ACS with transient ST elevation (unstable angina may have transient ST elevation)
3. Though early repolarization may change over months, if it changes from one ECG to the next on the same day, it is probably not early repol.
4. Use the equation to help you differentiate early repol from LAD occlusion.