A man in his 40’s presented with severe back pain radiating to the chest. Here was his ECG, with pain:
 |
| What is your diagnosis? |
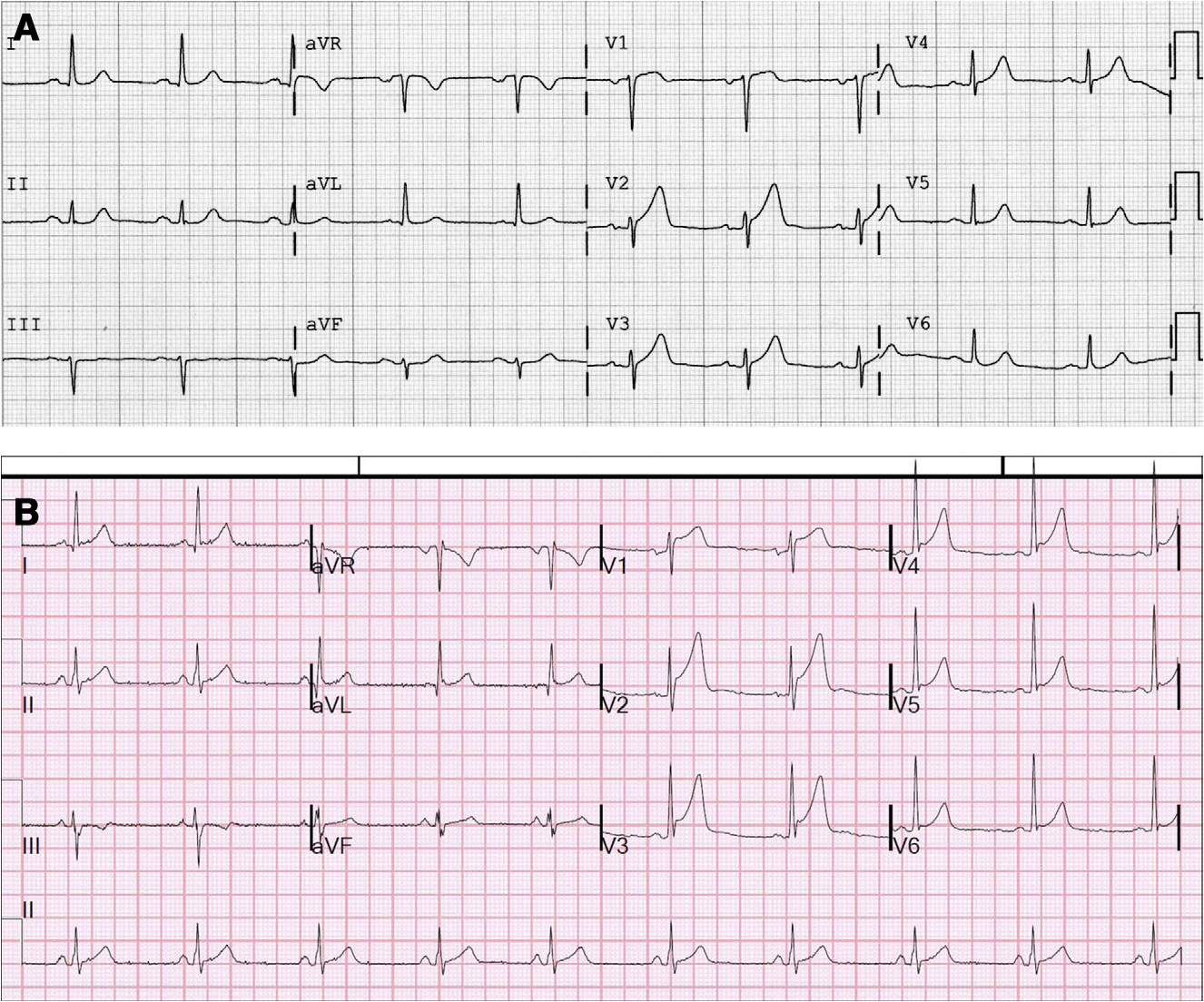
This is diagnostic of hyperacute T-waves and LAD occlusion or subtotal occlusion. There are subtle de Winter’s T-waves in V4-V6, in which the large T-wave is preceded by ST depression.
Apparently, it was not recognized (which is not unusual, this is subtle and difficult). Aortic dissection was on the differential diagnosis, and a CT of the chest ruled this out. Troponins were negative, the pain was resolved, and the patient was discharged.
He returned the next day with 9/10 back pain. Here was his ECG:
 |
| What do you think? |
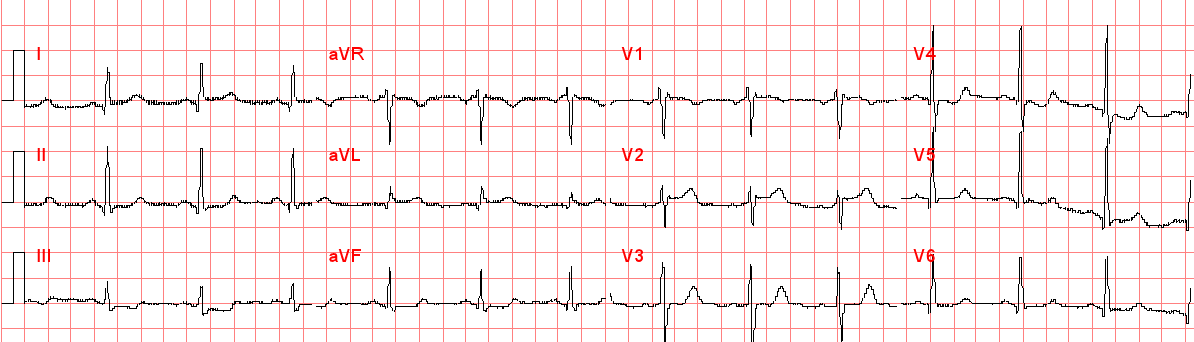
The fact that the T-waves are so different from the previous day’s confirms the ischemia of the previous day. There is ST segment elevation in precordial leads. Is it normal variant ST elevation (“early repolarization”)?
Even without a previous ECG for comparison, this is unlikely to be normal STE because of the poor R-wave progression. In our study of early repol vs. subtle anterior STEMI, only 5% of early repol had an average R-wave amplitude from V2-V4 of less than 5 mm. Here it is 1 + 2 + 9 = 12 divided by 3 = 4mm average. If you use the formula (see sidebar) which incorporates the ST elevation at 60 ms after the J-point in lead V3, and the QTc (393ms), then the result is 23.8, which is greater than 23.4 which indicates anterior STEMI.
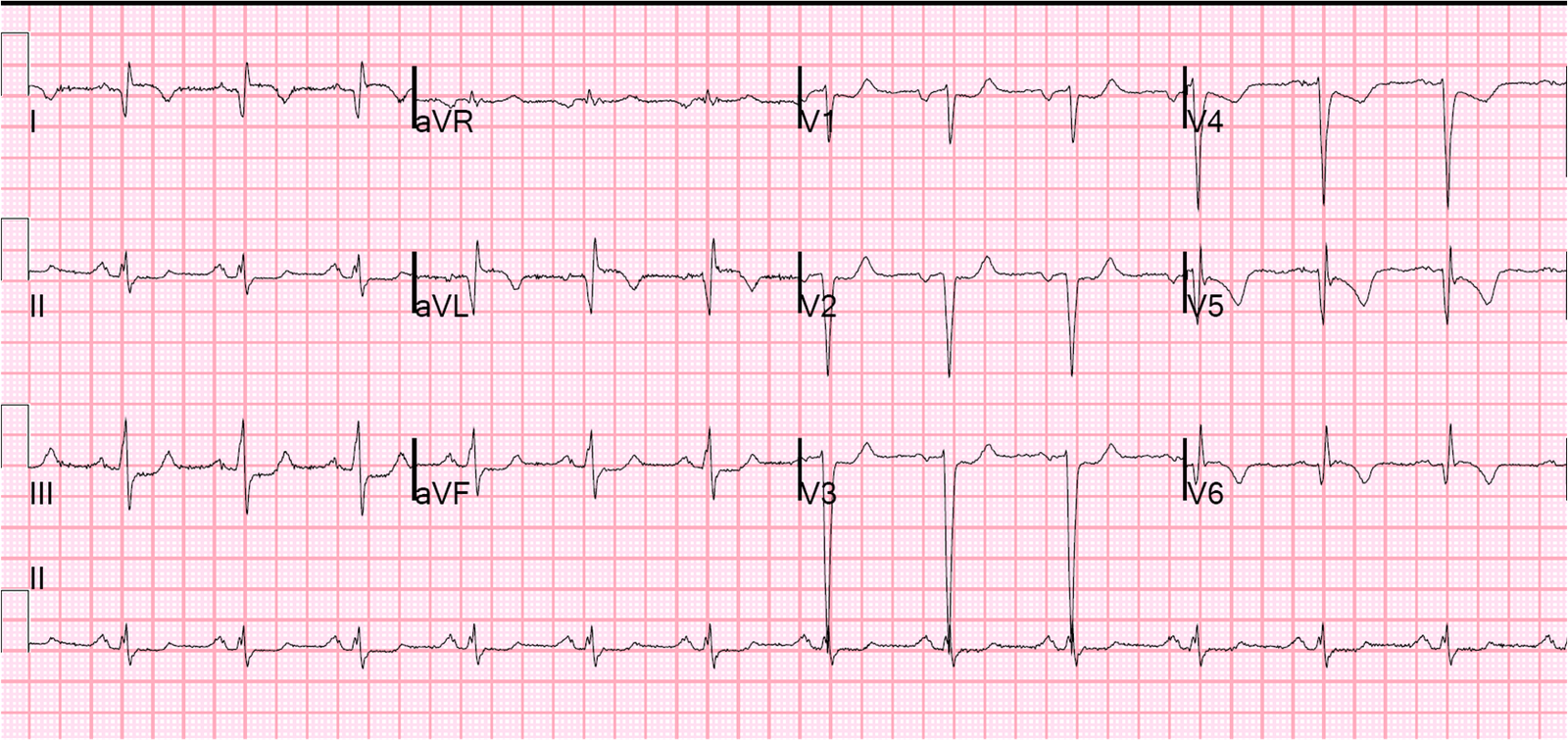
His pain resolved spontaneously, and he had the following ECG:
 |
| This is now obviously diagnostic of MI, and with T-wave inversion and absence of pain, the artery is likely to be open. The Q-waves indicate that the MI has probably been going on for quite some time. |
The troponin returned positive this time and the patient went for cath and had subtotal stenosis of the LAD just distal to the first diagonal. It was stented.
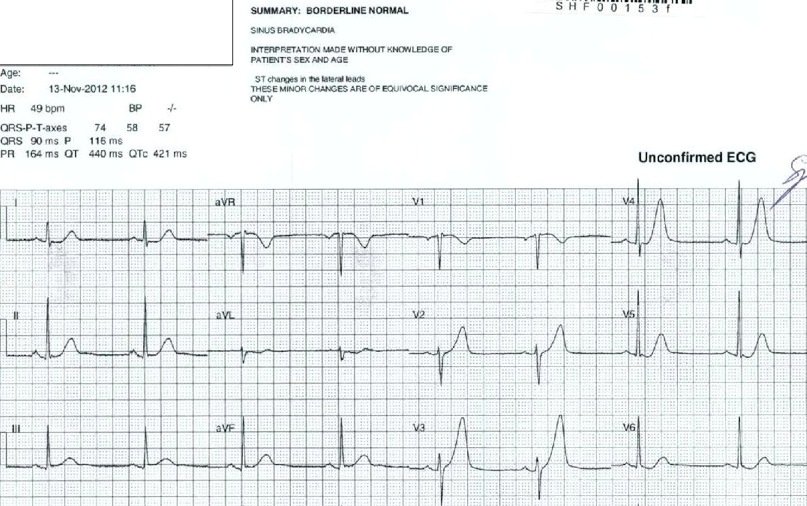
I don’t know the peak troponin, or echo results, or how much myocardium was lost. But here again is a “NonSTEMI” that really should be treated like a STEMI. The ECG 1 week later is consistent with significant myocardial loss:
 |
| Near total loss of R-waves from V2-V4 |