
A male in his 70’s with no h/o MI or CAD presented with new onset chest pain. Here is his ED ECG:
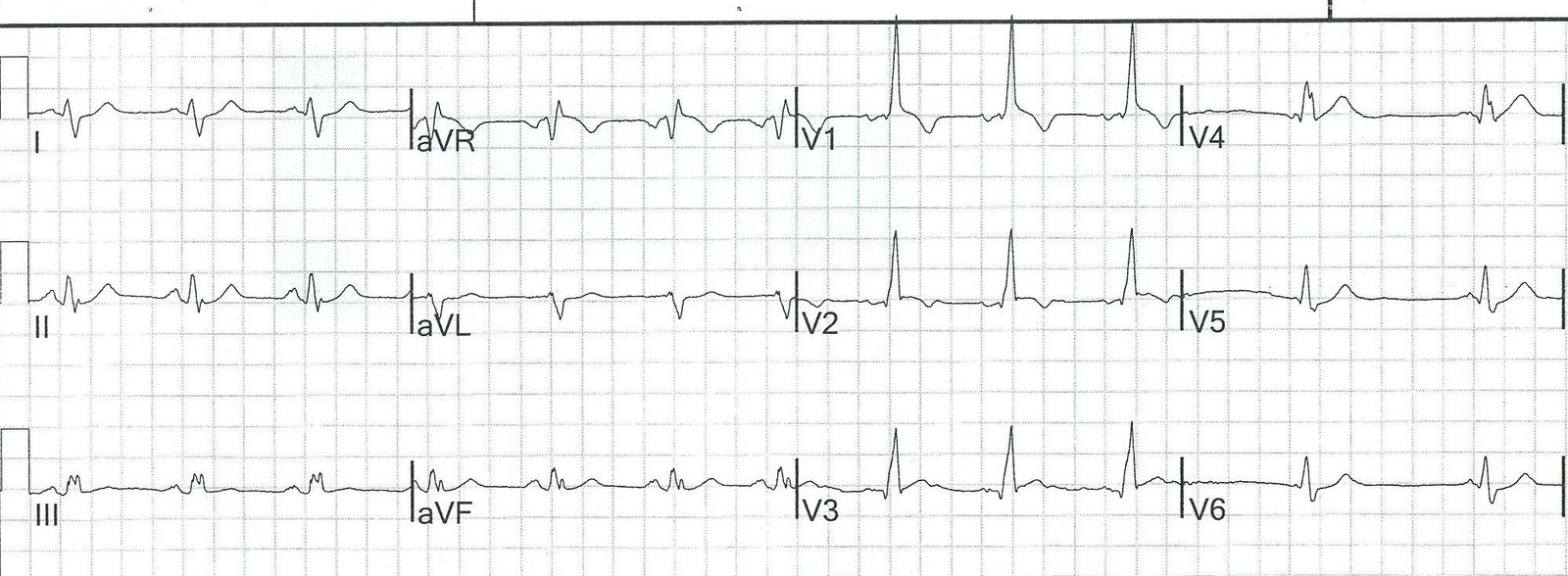 |
| There is sinus rhythm and right bundle branch block, and ST elevation in V1-V3. |
Normally, RBBB has ST depression in right precordial leads, especially
V2 and V3 (see ECG below). Sometimes it is isoelectric. But if there is any ST segment
elevation, as in this case, it is STEMI (or RBBB with old MI and persistent ST elevation) until proven otherwise.
 |
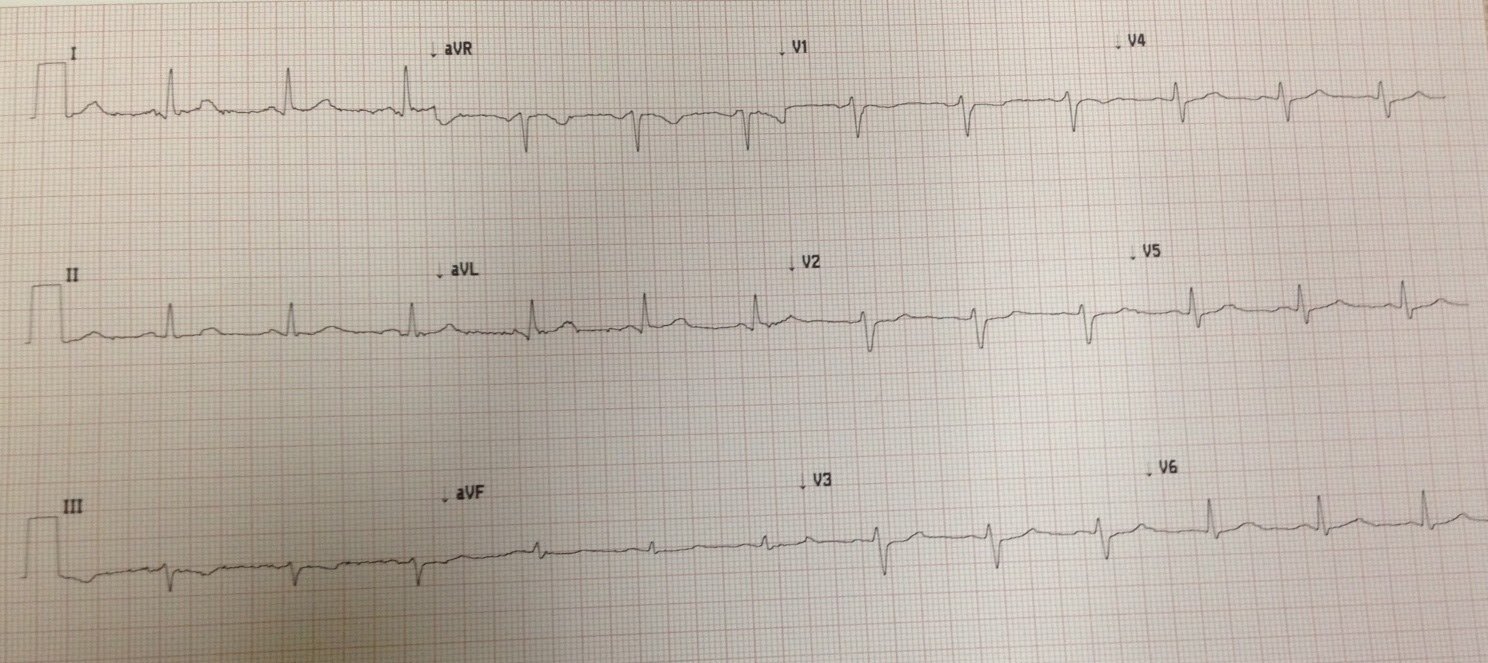
| Baseline RBBB (normal RBBB, no STEMI). Note that there is a large R’ wave in V1-V3 and discordant (opposite direction of QRS) ST segments. (Thanks to K. Wang’s EKG Atlas for this image) |
The emergency physician was very worried about STEMI, called the cardiologist on call, and they performed an immediate bedside echo which confirmed absence of anterior wall motion. Immediate angiogram was done and confirmed LAD occlusion, which was opened and stented.
Here is another example.
Here is a 3rd example.
Here is a 4th example.

{kind=link}