This was provided by Casey Parker at Broome Docs Blog, with permission.
A 23 year old presented with pleuritic left chest pain radiating to the left arm. He had a recent sore throat.
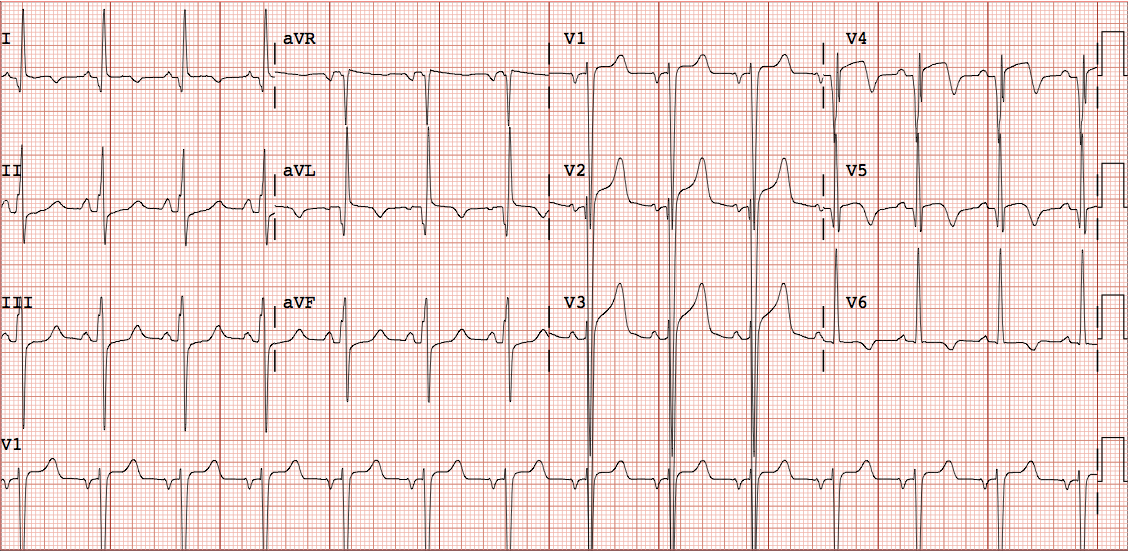
Here is his ECG:
 |
| Sinus rhythm with inferolateral ST elevation. There is no ST segment depression in aVL. Therefore, it is highly unlikely to be inferolateral STEMI. Correspondingly, the ST elevation in lead II is greater than lead III. There is slight ST elevation in lead I. The ST axis is directly towards lead II, and thus also V5. |
Along with the age, pleuritic chest pain, and viral symptoms, there is no doubt that this is peri- (or myo-) carditis. Occasionally, pericarditis can be localized to one wall or the other, in which case the ST elevation is also localized, as in MI, and it can mimic STEMI. Most pericarditis is diffuse, covering the entire epicardium, and thus the sum of the ST vectors is towards lead II.
We compared the ST segments of patients with early repolarization, pericarditis, and inferior STEMI, and found that ST depression in aVL was nearly perfect at distinguishing the benign entities from STEMI.
Of course, no rules are perfect, and if this patient had more typical pain and/or were a bit older, or had a positive troponin, I would get a stat echocardiogram to be certain there is no wall motion abnormality.
The initial troponin (they say troponin T??) was 0.88 and rose to 16 (which is very unusual for Trop T, so maybe they meant troponin I). An echocardiogram showed no wall motion abnormality.
Thus, the diagnosis is myocarditis.