A 90 yo with a history of orthostatic hypotension had a near syncopal event followed by chest pain. Chest pain was resolved upon arrival in the ED.
His previous ECG was normal.
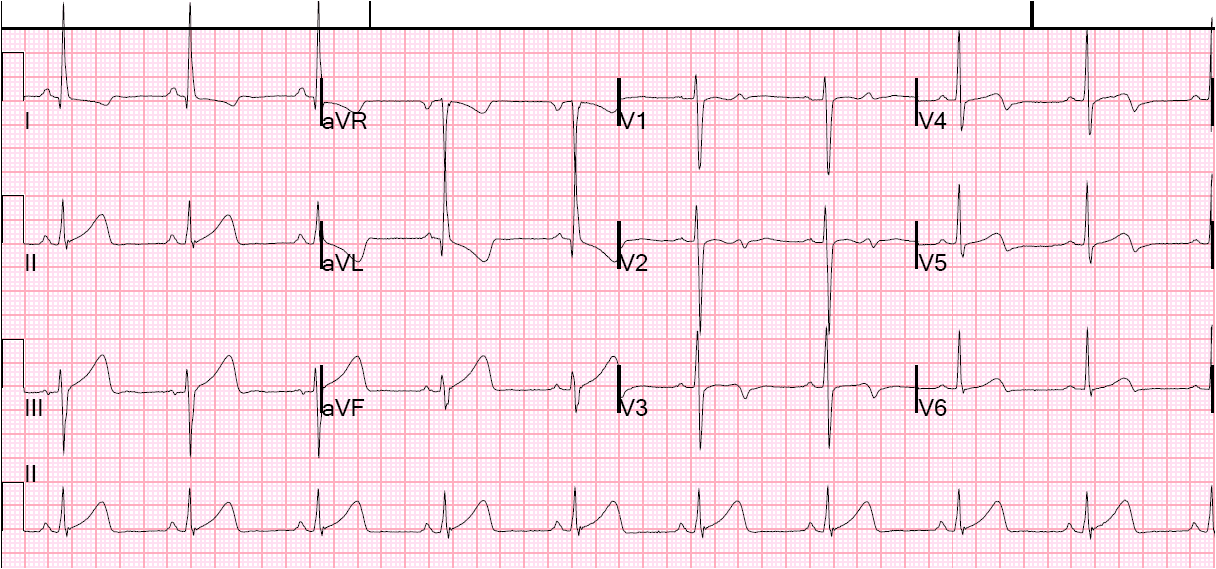
Here is his initial ECG:
 |
| There is a wide complex regular rhythm at a rate of about 80. What is it? Answer below. |
| There are no p-waves before each QRS, but there are inverted p-waves aftert the QRS (see arrow). This is either a junctional rhythm with left bundle branch block, or it is accelerated idioventricular rhythm (AIVR, an automatic rhythm — not a reentrant one — initiated in the ventricles and which propagates retrograde and results in retrograde p-waves). If it initiates in the right ventricle, it will have the appearance of LBBB. Is there ischemia? Whether it is AIVR or LBBB, the rule of appropriate discordance applies, so there should be discordant ST elevation in leads V2 and V3, but there is not. In fact, there may be less than 1 mm of concordant ST depression in lead V3. But it is not conclusive. |
Idioventricular rhythm is a common “reperfusion arrhythmia.” In other words, after reperfusion therapy for STEMI, the appearance of AIVR is usually a good sign, meaning that the artery is reperfused.
Some would argue that it cannot be “idio” if it conducts to the atria. But by usage, even these are called AIVR. It is very important to not try to treat AIVR. In fact, especially if there is no conduction to the atria, suppression of AIVR may result it asystole. This is a safe rhythm and usually has reasonable cardiac output, as the ventricles have time to fill.
ECG Diagnosis is either:
1) junctional rhythm with new LBBB, and possibly ischemia
2) accelerated idoventricular rhythm with possible ischemia, and possibly related to restoration of normal perfusion.
3) AV nodal re-entry???? with rate-related LBBB. Our electrophysiologist, Rehan Karim, states he has ablated AVNR”T” (“T” because it is not tachycardia) in a 90 year old, and that he has seen rate-related BBB at very slow rates.
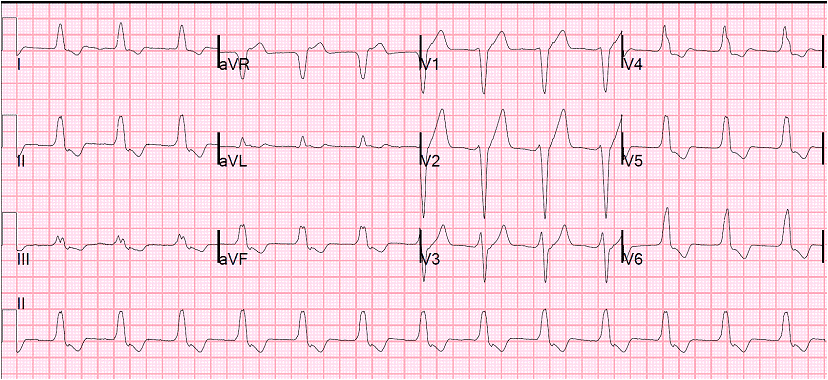
A repeat ECG had sinus rhythm at a rate of 54 and normal conduction (no LBBB), and was completely normal with no ischemia. The second explanation (AIVR), whether as a reperfusion dysrhythmia or not, seems most likely. The slow sinus rate supports the notion that this could be rate-related BBB.
The patient had a transient rise in troponin I from 2 values less than 0.012 ng/ml (undetectable) to 0.020 ng/ml (detectable but still below the 99% reference threshold).
Chest pain and possible ischemia were attributed not to ACS, but to transient hypoperfusion from orthostatic hypotension.
So there may have been 1) transient AIVR, or 2) junctional rhythm with transient or rate-related LBBB, or even 3) AVNRT with rate-related LBBB. Exactly how they relate to ischemia, chest pain, and reperfusion can only be speculated about.