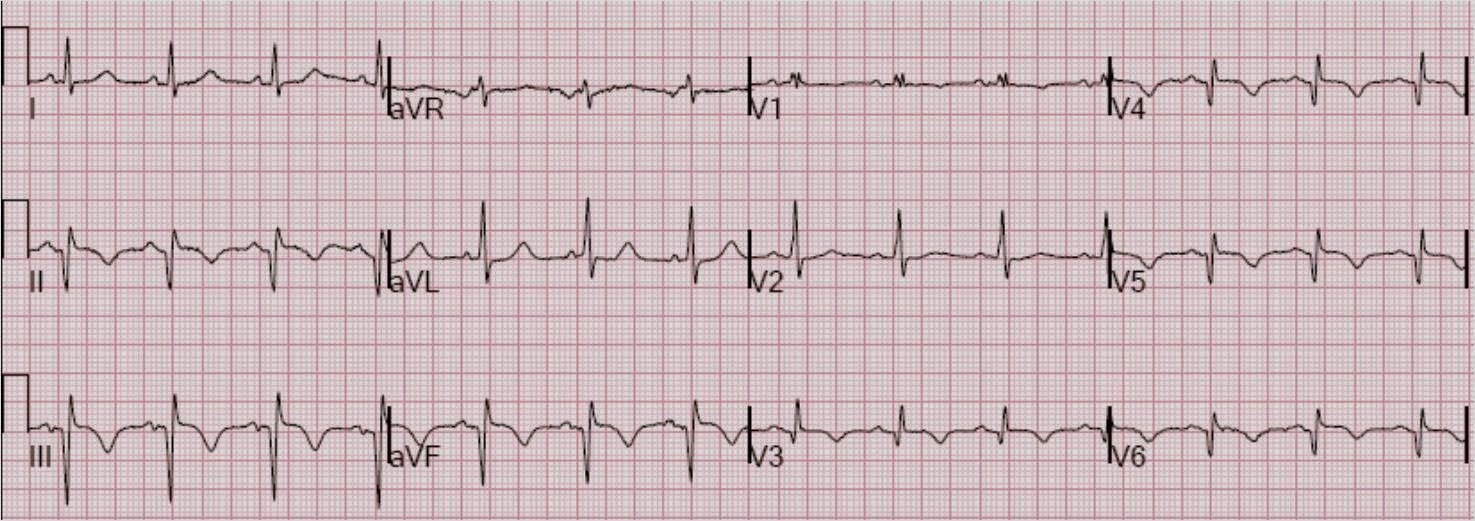
A 52 yo man began having substernal chest discomfort and presented 2 hours later. His prehospital ECG, which I cannot find, reportedly had some ST depression in precordial leads. He had this ECG recorded at 0658:
 |
| There are hyperacute T-waves in V1-V4. There is minimal ST elevation, almost 1 mm in V2 and less than 0.5 mm in V3, but this is diagnostic of anterior STEMI even without ST elevation. Using the equation (which may not be applicable because there is not enough ST elevation to even qualify for early repol), and the computerized QTc of 424, the value is 25.995 (greater than 23.4 is LAD occlusion). |
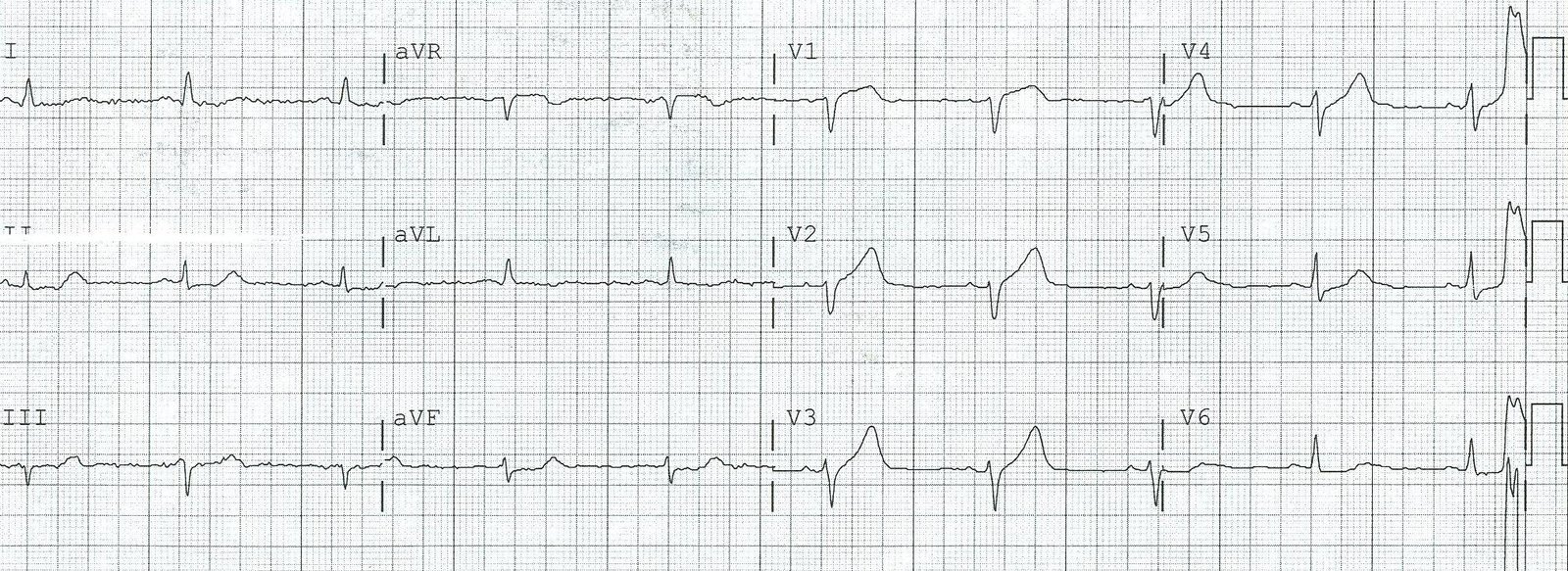
The clinicians who saw this patient do not, like me, spend their lives analyzing the minutiae of ECGs, so they were not certain of the diagnosis, but they did suspect it, so they did the entirely appropriate management of obtaining serial ECGs, and a repeat ECG was done at0713:
 |
|
| Still suspicious for hyperacute T’s but no ST elevation or significant evolution. The T-wave in V2 is less prominent, suggesting some reperfusion. QTc is 436 and equation remains greater than 23.4 |
So another was recorded at 0720:
 |
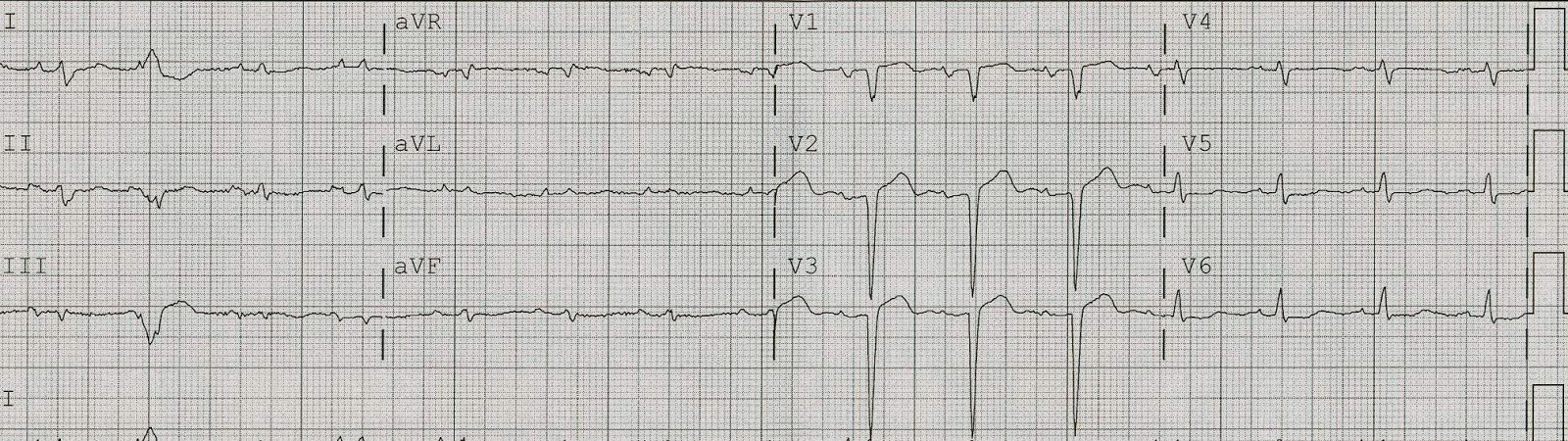
| Now there is ST elevation in V2 and V3, diagnostic of LAD occlusion |
Another at 0726:
 |
| Not much changed |
Another at 0744:
 |
| Now it is unequivocal |
At this point, the cath lab was activated.
This is the post cath ECG:

Cath showed a complete mid-LAD occlusion. Peak troponin I was 120, even with a short door to balloon time, and even though the initial ECG was not striking. The echo showed a large anteroapical wall motion abnormality.
I suspect the prehospital ECG had de Winter’s ST depression and T-waves.