This is a 45 yo male who had an inferior STEMI 6 months prior, was found to have severe LAD and left main disease, and was supposed to be set up for CABG a few weeks later, but did not follow up.
3 hours prior to calling 911 he developed typical chest pain.
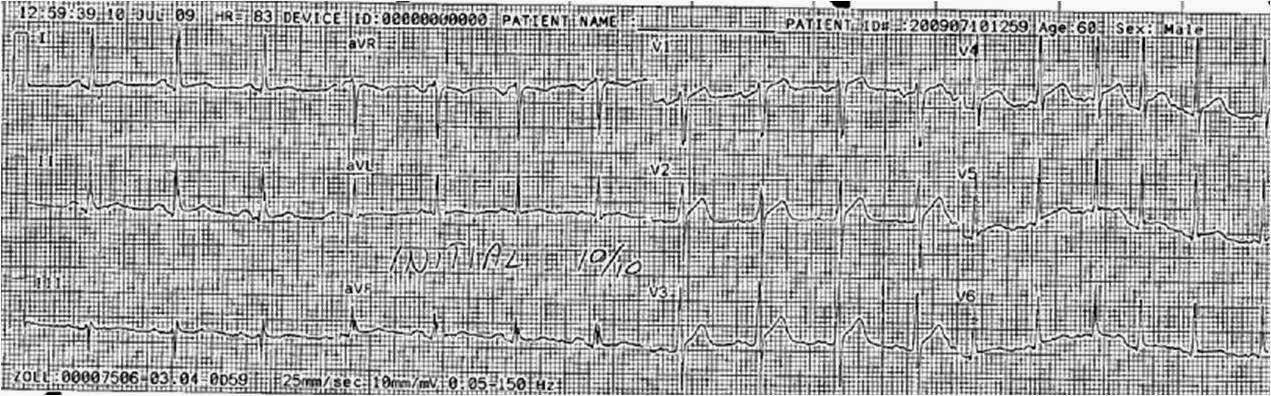
The medics recorded this prehospital ECG at 1535:
 |
|
|
How can one decide whether this is ER or MI? First, if an old ECG is available, then compare. Only rarely does early repolarization change from date to date, though it is possible.
Second, I have developed a score that helps to differentiate the two. His BER score, based on ST elevation at 60 ms after the J-point in lead V3, QTc (400), and R-wave amplitude in V4 is 23.9 (greater than 23.4 is likely anterior STEMI).
(1.196 x STE60 in V3 in mm) + (0.059 x computerized QTc) – (0.326 x RA in V4 in mm)
Third, one can do an immediate cardiac ultrasound.
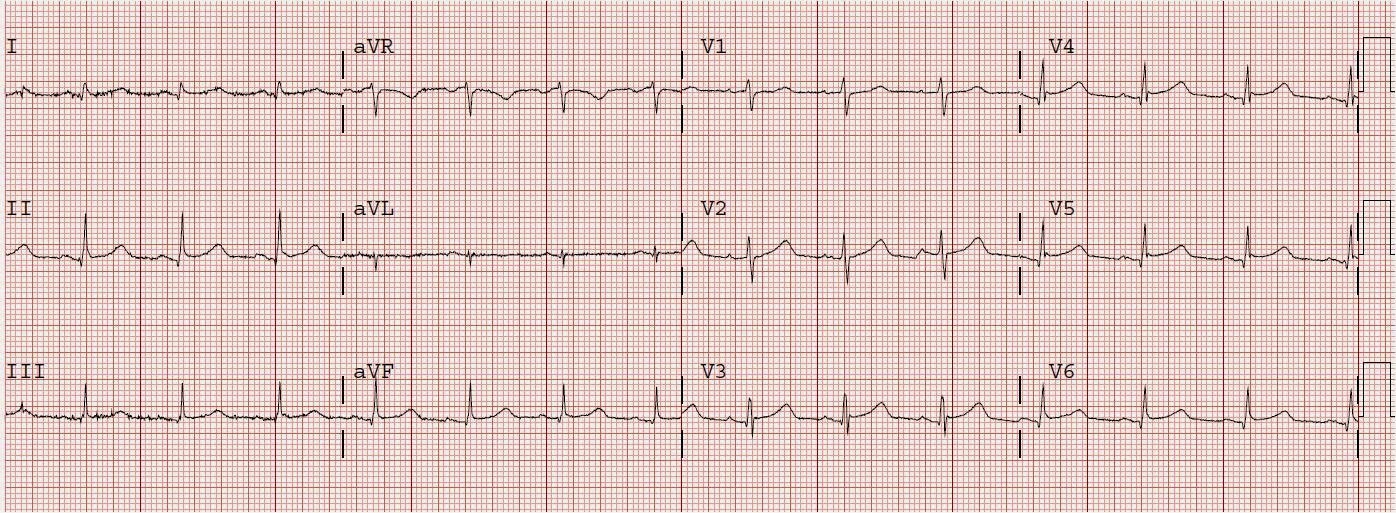
Medics gave him nitroglycerine sublingual and his pain resolved. He arrived in the ED and had this ECG recorded at 1544
 |
|
|
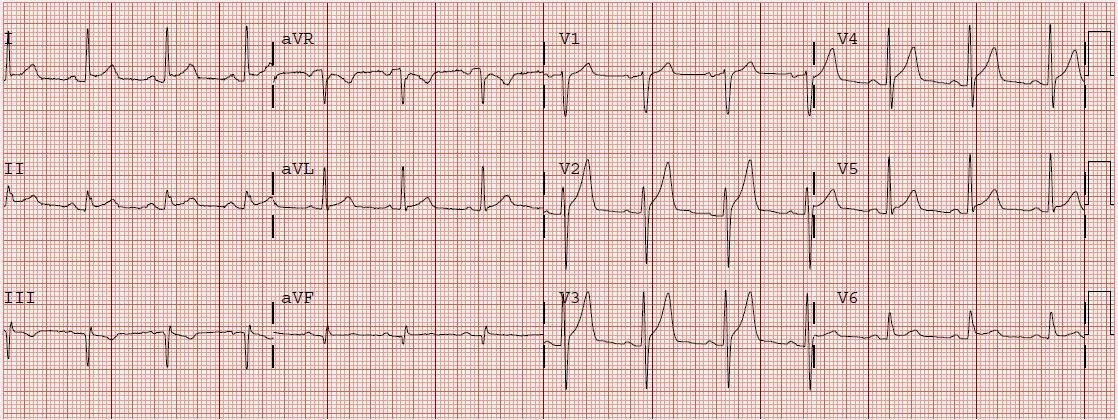
A previous ECG was found:
 |
|
|
The patient remained pain free, and this ECG was recorded at 1606:

He remained pain free. A bedside ultrasound was done by an emergency physician and simultaneously read by a cardiologist. They could see no anterior wall motion abnormality. Diagnosis of ACS was in doubt.
His old angiogram was reviewed and it was known that his disease was not amenable to PCI. He needed CABG. He was therefore treated with eptifibatide, heparin, and aspirin, and referred for CABG, but not immediately.
The next AM, this ECG was recorded:
 |
|
|
 |
|
|
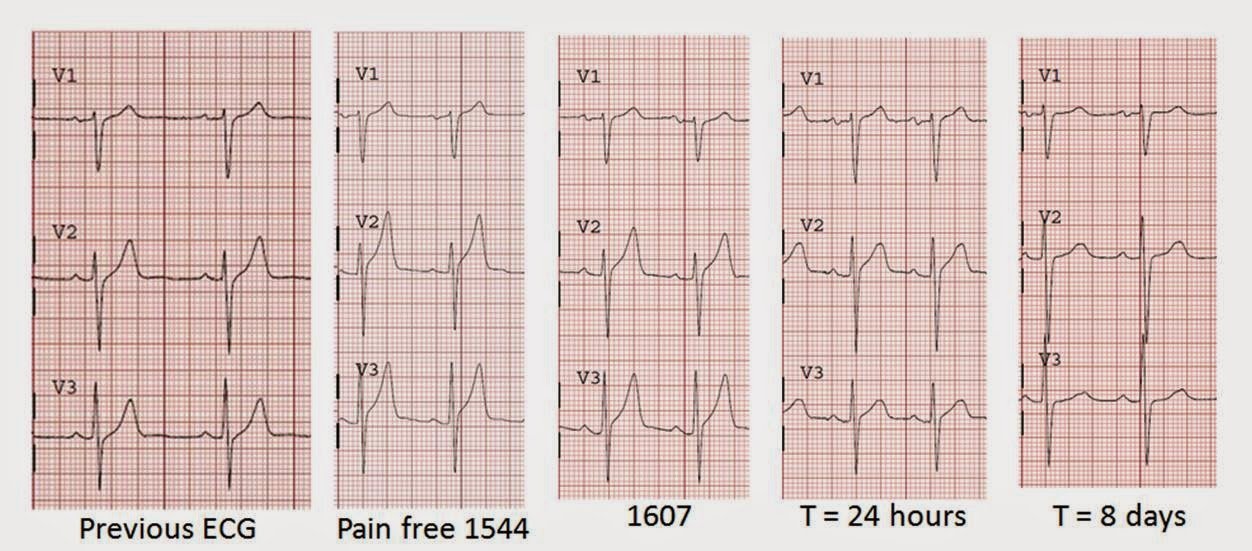
It is often difficult to see changes unless they are directly side-by-side. Here are V1-V3 from start to finish. I did not include the prehospital because it is identical to the first ED ECG:
 |
|
|
All troponins were undetectable (less than 0.04 ng/ml).
The patient had a critical LAD stenosis. Flow had spontaneously been restored, perhaps aided by nitroglycerin. He underwent CABG.
Conclusions:
1. Anterior STEMI can look very much like early repolarization. There are means to distinguish the two.
2. Transient ST elevation is very hazardous. Even when the serial troponins are negative, the ECG is critical to the diagnosis of ACS.
3. When flow is restored, wall motion may completely recover so that echocardiogram does not detect the previous ischemia.
4. This is not pericarditis because:
a. Pain was typical for MI (substernal, not postional or sharp, resolved with NTG)
b. There is relative reciprocal ST depression in lead III.
Pericarditis does not have reciprocal depression.
c. ST elevation of pericarditis is maximal in leads II and V5, V6.
Here the ST elevation is maximal in V2-V4.
d. Pericarditis does not have hyperacute T-waves.
e. Tight proximal LAD stenosis explains STE in precordial leads and I and aVL.