I had a recent comment on this post, which was put up 7 years ago (850 posts since then!). I was reminded of it. And so I thought I would repost it.
Case
This is a 48 y.o. male with a history of Bipolar disorder, polysubstance abuse, spontaneous pneumothorax x2, who presents for chest pain x 4 hours. The patient was in his usual state of health until this afternoon when he noticed the gradual onset of bilateral chest pain. He had a relapse of crack use this AM. He describes the pain as bilateral, radiating to the left arm, worsening over time, and associated with mild SOB and also some pleuritic chest pain. There is no relation of pain to exertion or meals, and no associated diaphoresis, nausea or vomiting. No recent long sedentary periods. No recent trauma, but has been doing more manual labor than usual. Pt has not had chest pain with crack use before.
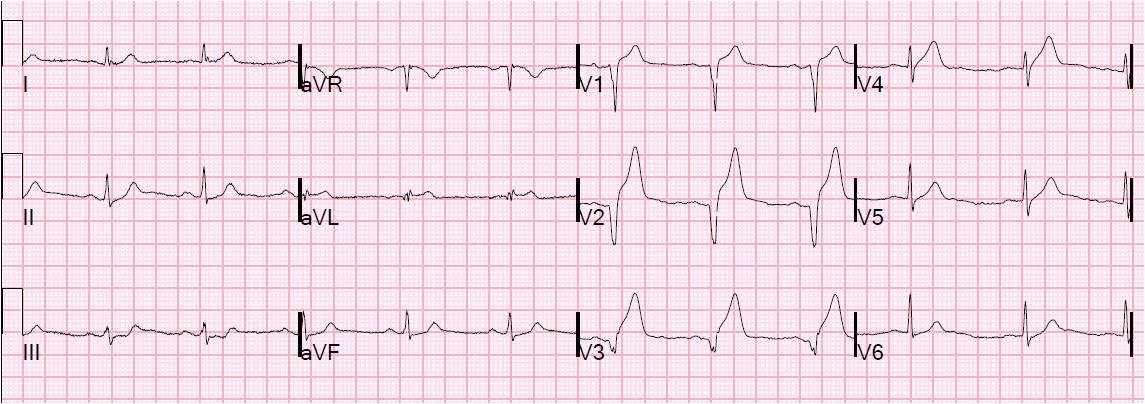
Here is his initial ECG:
 |
|
|
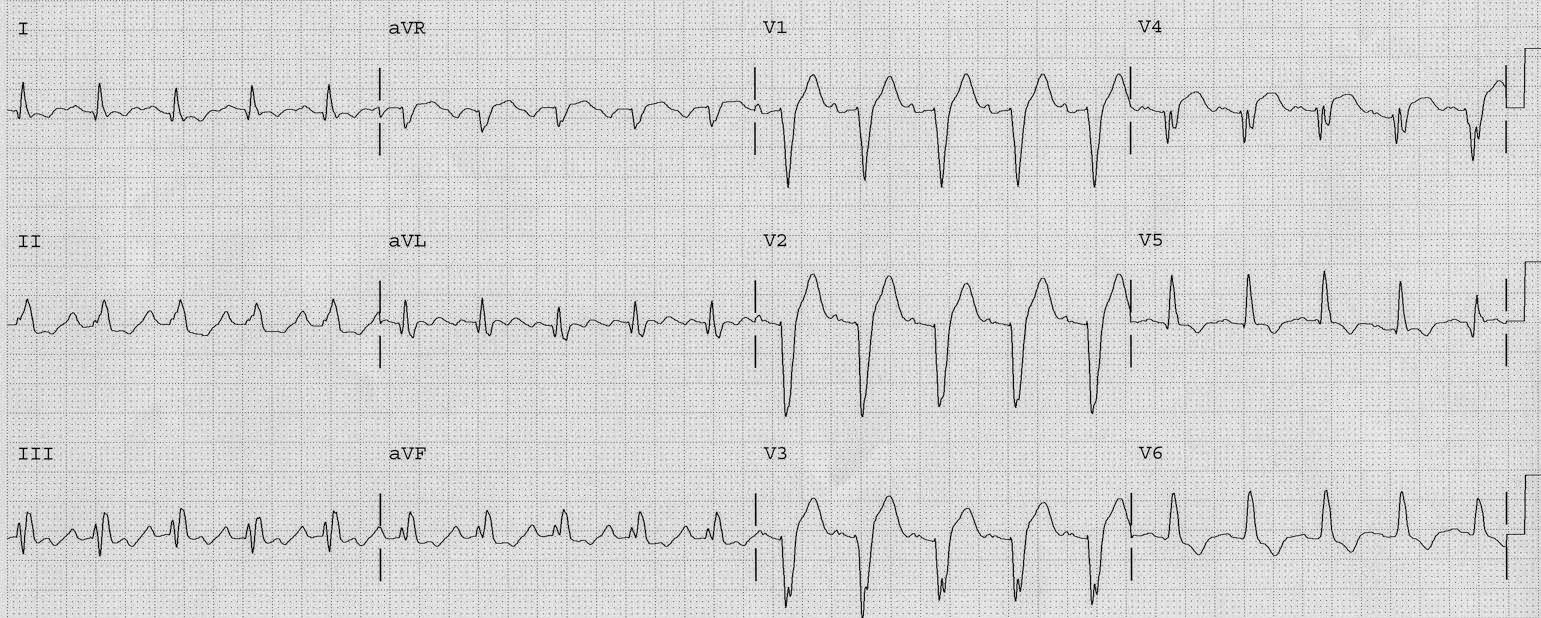
Here is his previous ECG for comparison, recorded 7 months prior:
 |
|
|
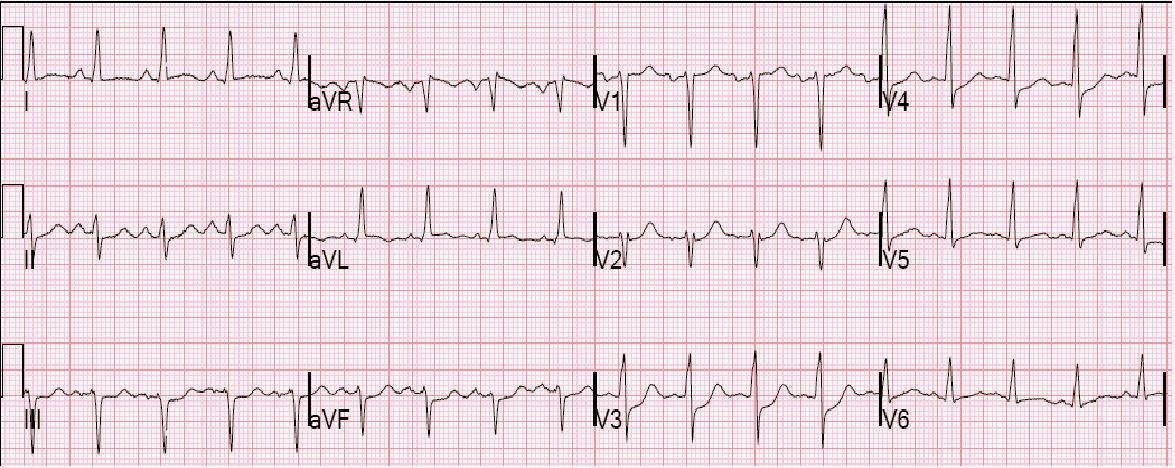
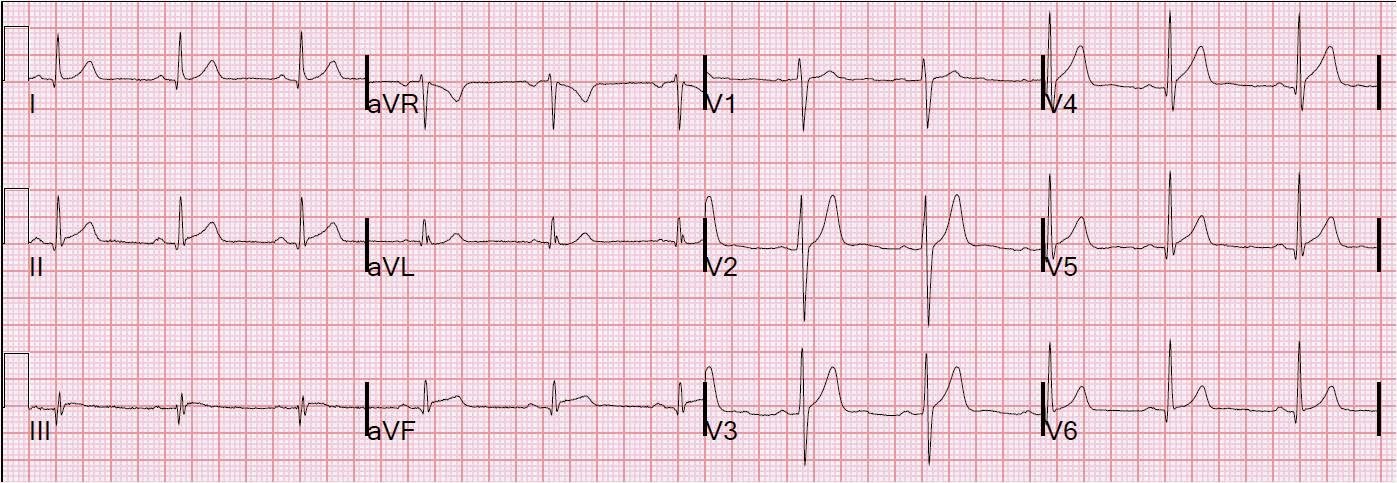
Here I place them on the same page for better comparison:
 |
||
|
Here I have magnified II, III, aVF, and aVL for better comparison:
 |
|
|
Here I have magnified V1-V3 for better comparison:
 |
|
|
The Emergency physician started therapy for NSTEMI. The first troponin returned at 2.25 ng/mL. The cardiology fellow then opined that this was myopericardititis and instructed to stop the heparin. However, myopericarditis is a diagnosis of exclusion and much less common than acute MI. One must undertake treatment for ACS, including an angiogram. Only if the angiogram is normal would one then consider myocarditis and probably obtain an MRI.
The reciprocal ST depression in lead aVL and the T-wave enlargement in V2 and V3 are all but diagnostic of MI.
Follow up:
The troponin I peaked at 23.6 ng/mL. The echo showed an inferior and anterior wall motion abnormality. Thus, it was not pericarditis, though myocarditis is possible.. Angiogram showed a ruptured plaque in the proximal LAD, with distal embolization of thrombus to the apex. This was a “type III,” or “wraparound” LAD which supplies both anterior and inferior walls. This accounts for the transient hyperacute T-waves in anterior leads and for the ST elevation in inferior leads.
Even without the angiogram, the rapid rise and fall of troponin is highly suggestive of MI, not myopericarditis.
The stenosis was minimal, and the ACS occurred in the setting of cocaine use, so the therapy was eptifibatide and heparin for 72 hours, with no PCI.
Learning Points
1) Pericarditis should never be assumed when there is even a hint of reciprocal ST depression. Only localized pericarditis (most pericarditis is “diffuse” inflammation of the entire pericardium) ever has reciprocal ST depression, and localized pericarditis is very rare. I suspect that many cases of “localized pericarditis” are really STEMI that went undiagnosed.
2) Wraparound or Type III LAD ACS mimics pericarditis because it leads to diffuse ST elevation.