For other cases of cardiac arrest, see these posts
Case
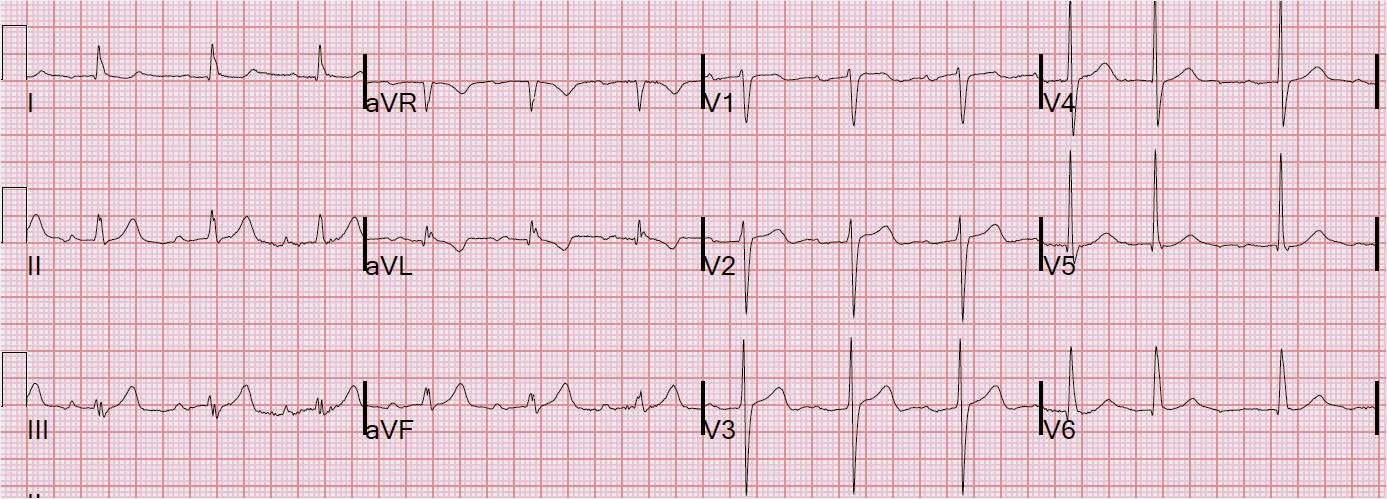
This 200 kg patient was watching TV when he had a witnessed v fib arrest, and had a prolonged resuscitation. In the ED, his pH was 7.20, K of 4.9, and this was his initial ECG:
 One might be tempted to diagnose ventricular tachycardia. However, there are p-waves best seen in lead I, with a slightly long PR interval. There are also PVCs which are unlikely to occur during V tach.
One might be tempted to diagnose ventricular tachycardia. However, there are p-waves best seen in lead I, with a slightly long PR interval. There are also PVCs which are unlikely to occur during V tach.
.
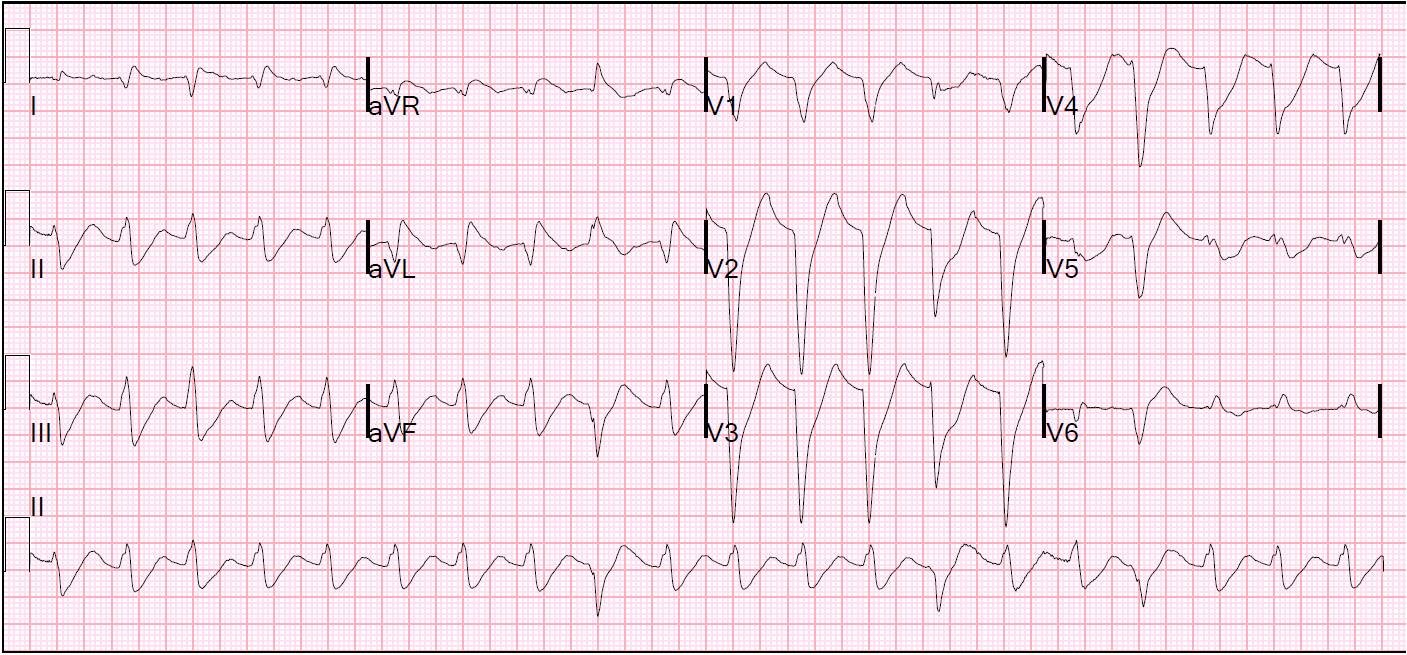
Once it is determined to be sinus tach (with aberrancy, in this case a slightly unusual LBBB), one must find the end of the QRS (J-point, the start of the ST segment) in order to find the ST segment and to evaluate for ST elevation or depression. In this case, the end of the QRS is easily found in lead V6. Then, draw a line through that J-point an extend it up and down. I have done this in detail in this previous case:
https://drsmithsecgblog.com/2010/11/wide-complex-tachycardia-its-really.html
Here are the lines for this ECG:
 Then you can find the end of the QRS in any lead. After doing so, you can see profound concordant ST depression in leads V2-V5, and Concordant ST elevation in I and aVL with reciprocal ST depression in II, III, aVF.
Then you can find the end of the QRS in any lead. After doing so, you can see profound concordant ST depression in leads V2-V5, and Concordant ST elevation in I and aVL with reciprocal ST depression in II, III, aVF.
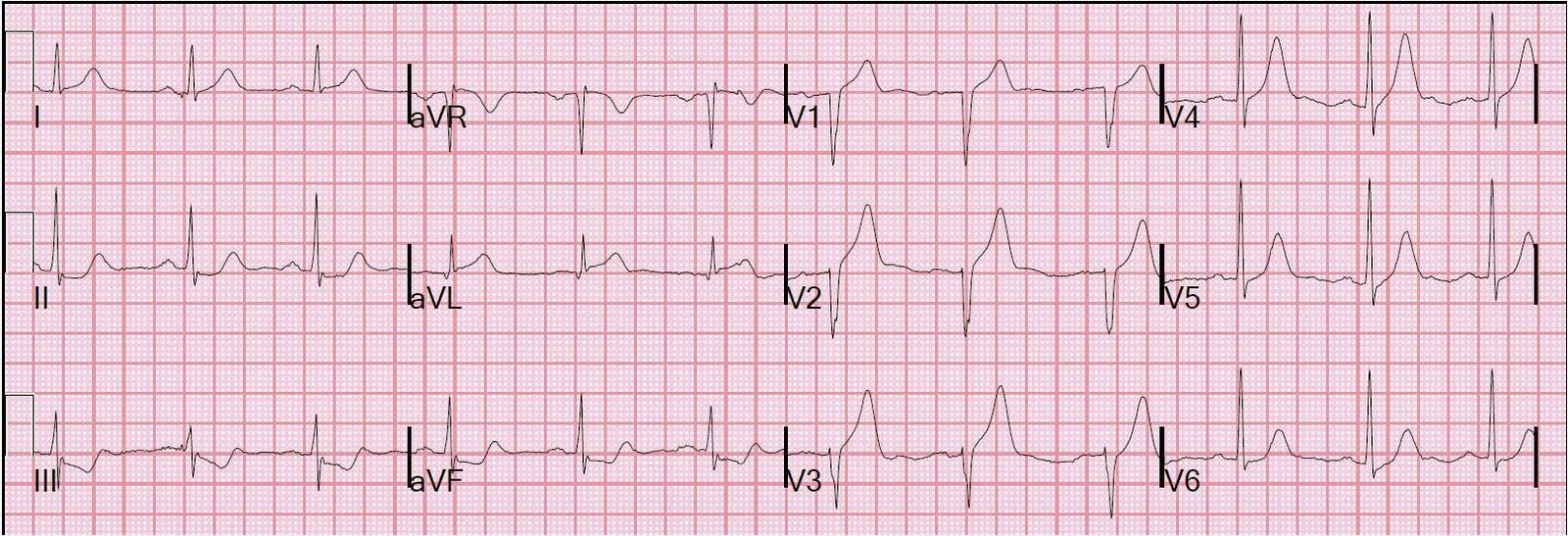
70 minutes after the first ECG, this ECG was recorded:

Now the QRS is narrower. The sinus rhythm is obvious. There is a R-wave in V6 typical of LBBB, but the ST segment is not discordant as it should be. Rather, it is concordant. V1-V3 have concordant ST depression.
The patient’s initial troponin was negative. Because of other factors, he was not taken for PCI. Troponin 5.5 hours later was 308. ng/ml. Echo was technically difficult but showed LVH and probable lateral wall motion abnormality. This was presumably a large posterolateral STEMI with LBBB.