This 58 yo male with a PMHx only significant for Sleep Apnea felt dizzy, lightheaded and nauseated after exerting himself, with no CP or SOB. He subsequently had a syncopal event and was down for 1-2 minutes. His wife called 911. EMS found him with an irregular heart rate at 200-250 beats per minute. He was electrically cardioverted to sinus rhythm. Upon arrival to the ED, he had the following 12-lead ECG:

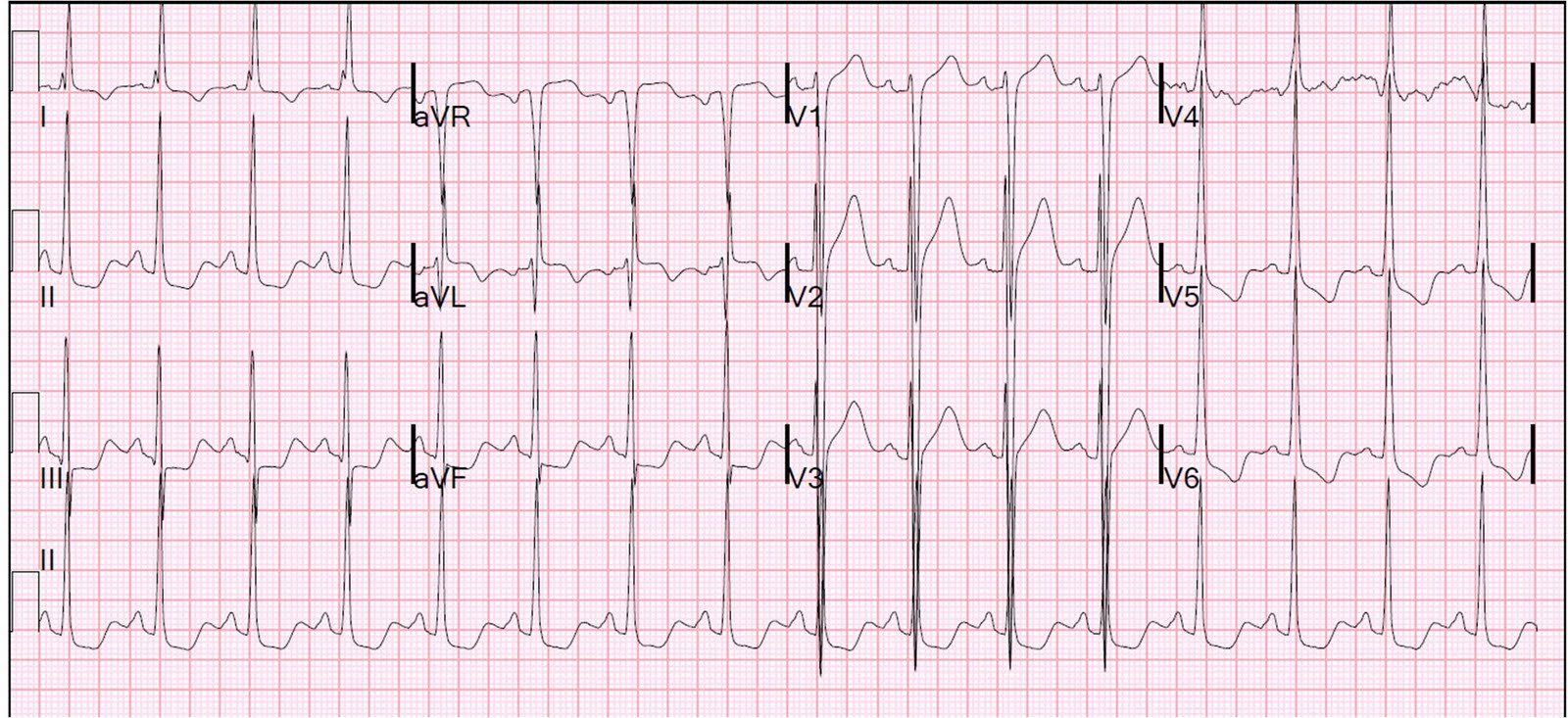
There is striking ST segment elevation in V1 and V2, with ST depression in V3-V6 as well as I, II, and aVF. There is also a wide QRS. One might think this represents acute STEMI, or Bundle branch block with discordant ST segments and suspicously concordant T-waves.
However, closer inspection reveals a very short PR interval and that the wide QRS is due to a slurred upstroke (delta wave).
This is WPW, which is well known to produce pseudoinfarction patterns.
The patient had a positive troponin, underwent cath which showed completely clean coronaries, and then underwent EP testing which revealed that, in atrial fibrillation, he has an R-R interval as short as 220 ms, which is dangerously short. Ablation was planned for a later date.