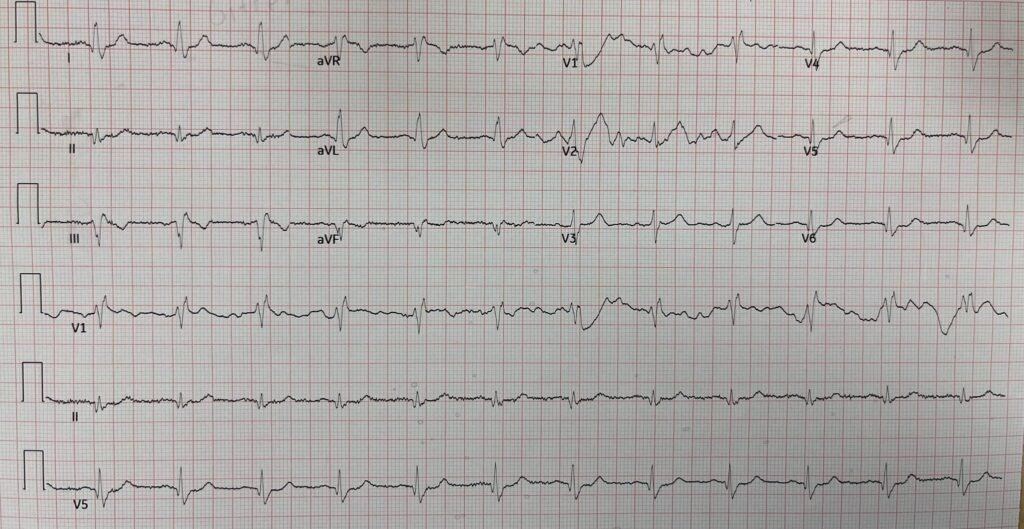
An 85-year-old man with a history of MI with stents woke up feeling unwell. He reported that the original sensation was difficult to describe, but that he subsequently developed chest pain. He called emergency medical services, who activated ALS helicopter transport to a PCI center non-emergently. This was the first ECG recorded by the team in the helicopter (ECG 1, time unknown):
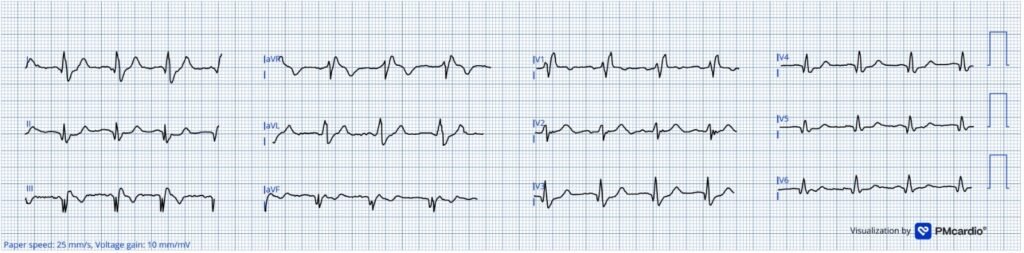
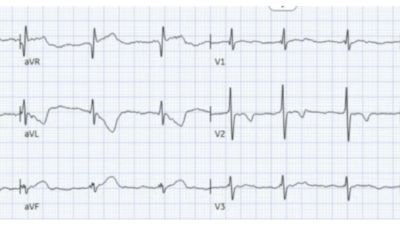
There is sinus rhythm with RBBB. There are Q waves in the inferior leads suggestive of MI and consistent with the patient’s history, but there was no available baseline tracing to confirm that these Q waves were old. There is anterior ST depression maximal in V3-V4 which can be seen in RBBB alone, but only if discordant to the terminal part of the QRS. Thus, it is especially concerning in this case because there is no R’ wave in V3-V4 and these leads have terminal T wave positivity (See this post for more). On its own, this ECG is suspicious of acute OMI and warrants extreme caution with repeat ECG monitoring if not immediate cath lab activation.
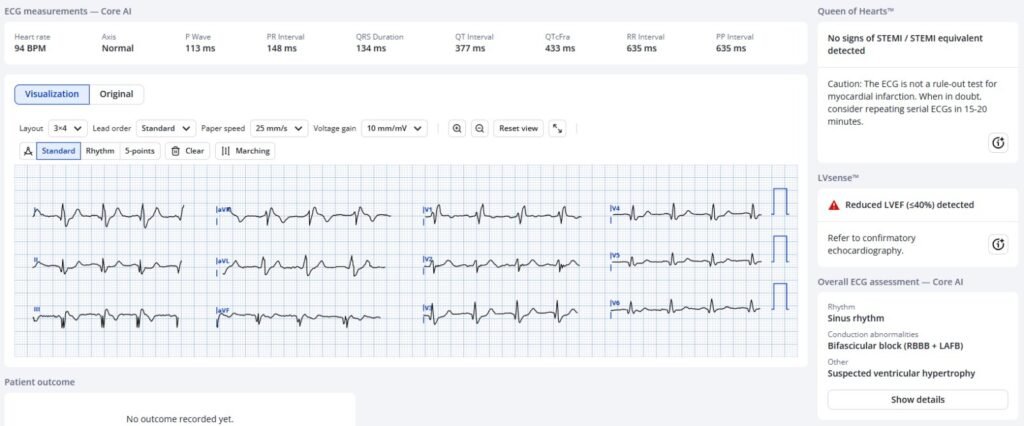
The Queen of Hearts does not see OMI here. This may be due to the combination of RBBB and Q waves which are both reasons a patient may have ST segment deviation without OMI:
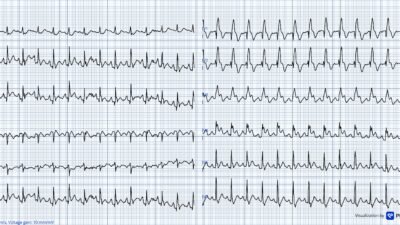
The diligent flight medics recorded ECG 2 an unknown amount of time after the first:
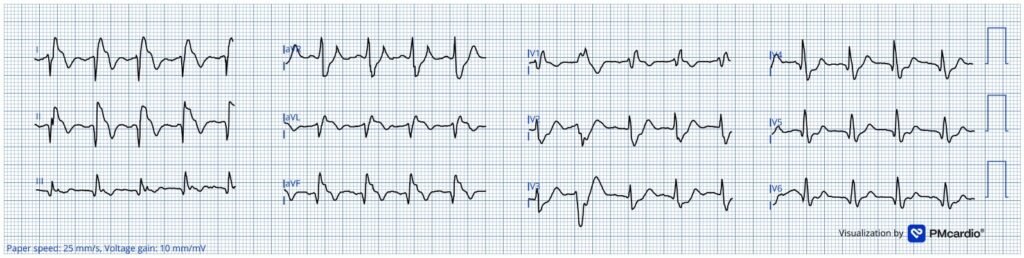
As compared with ECG 1, there are dramatic changes. There is increased ST depression in the anterior leads, diagnostic of posterior OMI. There is also a strange territory of new ST elevation simultaneously in high lateral leads I and aVL and in inferior leads II and aVF, and the axis has shifted rightward. How can this have happened?
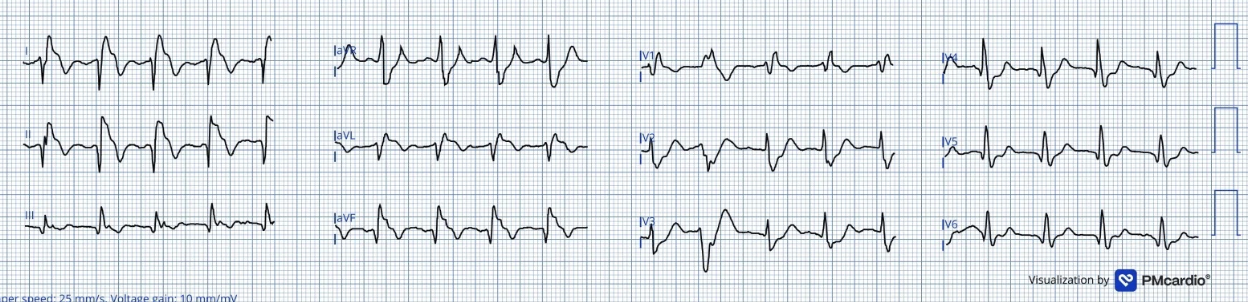
Transposition of the LA and RA electrodes: If the stickers or cables are swapped between the right and left arms, Wilson’s central terminal is affected such that the ECG records lead I upside-down, and swaps leads II and III, and leads aVR and aVL. Lead aVF remains unaffected. So what looks like new ST elevation in lead I is actually new ST depression. In fact, the entire ECG can be corrected by making the appropriate edits (thanks to Dr. Mark Hellerman for editing the ECGs for this case):
By correcting for the lead reversal an evolving inferior+posterior OMI becomes apparent.
The Queen does not see OMI in ECG 2 without correction for electrode transposition:

However, when the leads are corrected in ECG 2, the Queen does see OMI:

Case continued: The flight medics activated the cath lab upon seeing ECG 2 for “EKG changes en route”. It is unclear if they appreciated the electrode transposition, but they did not mention it to the receiving hospital.
The attending emergency physician receiving report of the incoming cath lab activation wrote “Given the patient’s prior history and presentation, working diagnosis on initial evaluation is unstable angina, EKG changes are dynamic on EMS EKG. Will obtain (another ECG) when here, discussed possible emergent cath with cardiology”.
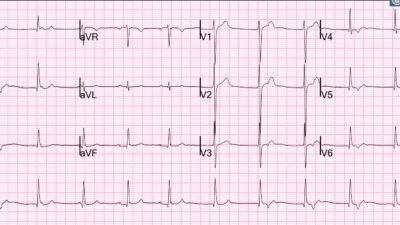
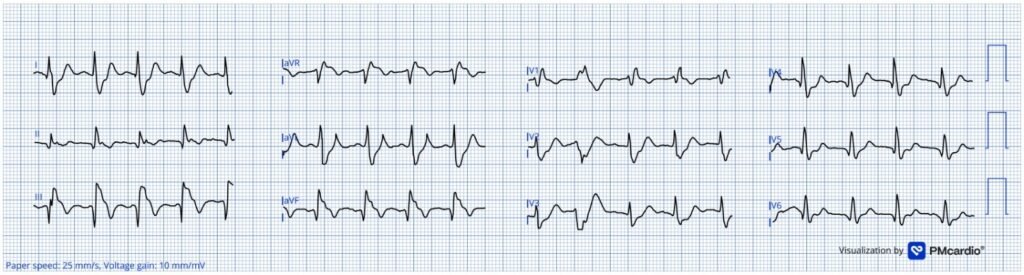
Upon arrival at the hospital, ECG 3 was recorded (status of the patient’s pain at this time is unknown):
The electrodes have this time been placed correctly. The ST depressions and elevations have largely disappeared, suggesting reperfusion.
Comparing this ECG with ECG 2, the attending ED physician and cardiologist who had come to the ED to evaluate the patient wrote “EMS EKG elevation in I, aVL resolved”. The patient was promptly placed on a heparin drip and sent to the cath lab for “dynamic EKG changes”, where the following lesions were found:
LMCA: 30%
Prox LAD: 50%
Mid LAD: 80%
Prox LCx: 90%
1st Diag: 90%
Mid RCA: 100%
It is impossible to know if this patient would have received the emergent catheterization he needed had there been no electrode transposition. It is possible, especially because no transposition seems to have been recognized during this case, that this patient was very lucky to have his ECG improperly recorded!
Learning points:
- Recognizing appropriate vs inappropriate anterior ST depression in patients with RBBB is a valuable skill in diagnosing OMI.
- Recognizing both the presence and effects of electrode transposition can explain otherwise bizarre ECG changes. Once the type of transposition is identified, the clinician can look past the error at the true ECG.
= = =
==================================
MY Comment, by KEN GRAUER, MD (5/29/2026):
We’ve encountered the “theme” of today’s case many times on Dr. Smith’s ECG Blog — namely, detecting the subtleties of what is “new” vs “old” vs “new superimposed on old” — with this detection made all the more difficult in today’s case by the presence of RBBB (Right Bundle Branch Block) and the absence of a prior tracing for comparison (See My Comment in the February 1, 2026 post for another example of RBBB with subtle findings and no prior tracing).
- I focus My Comment below on a few additional subtleties to those covered in Hans Helseth’s excellent presentation.
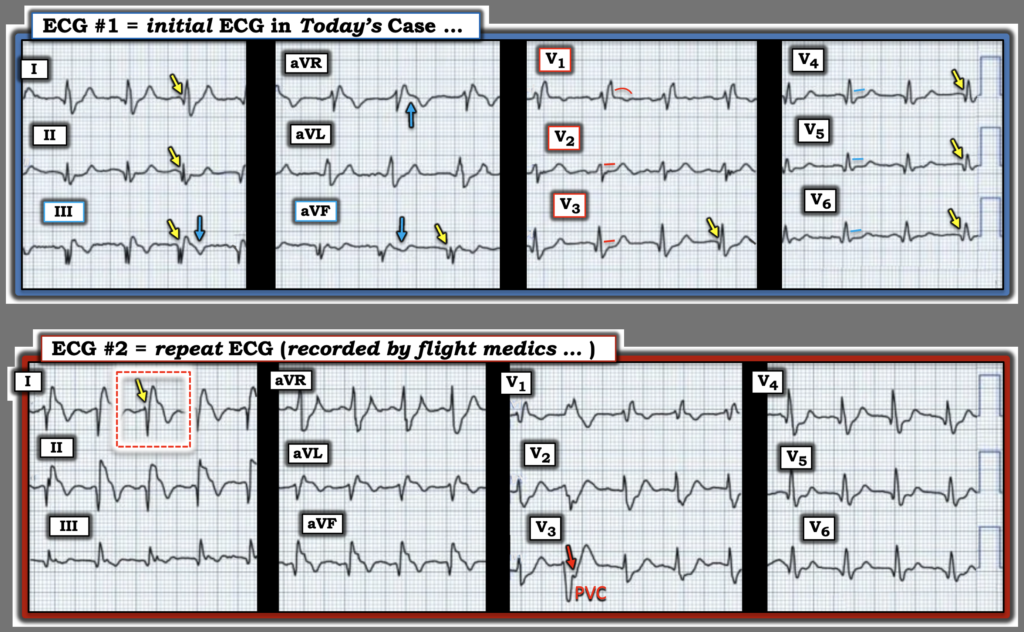
- For clarity in Figure-1 — I’ve reproduced and labeled the first 2 tracings shown in today’s case.
= = =
The Initial ECG:
Considering that today’s patient is an 85-year old man with known coronary disease — with a history that began with a “difficult-to-describe” symptom (that only later became chest pain) — and without ready availability of a prior tracing for comparison — I found it challenging to determine if the initial ECG in Figure-1 was indicative of an acute evolving event.
- Even certainty about the rhythm in this tracing is challenging — as P waves are not well seen in the limb leads — and the R-R interval shows slight variation. Alas, leads V1,V2 show regular P waves with a constant PR interval ==> this is sinus vs an atrial rhythm.
- As per Hans Helseth — the large inferior Q waves are clearly a marker of a prior inferior MI. Note especially the marked fragmentation in leads III and aVF (that result in a Q wave followed by a “pseudo-R wave” in these leads — indicative of “scarring” from this patient’s previous infarction).
- Infarction Q waves — are actually present in at least 7 (if not 8) of the 12 leads (YELLOW arrows in leads II,III,aVF; V3,4,5,6 — and the smaller, narrow q wave in lead I).
- Overall QRS amplitude is reduced (None of the 12 leads exceed 10mm — and QRS amplitude in most leads is significantly less than this, potentially a result of reduced LV function from prior infarctions).
- And, there is the aforementioned RBBB (as diagnosed by the rSR’ in right-sided lead V1 — and the wide, terminal S waves in lateral leads I and aVL — with a smaller, narrow s wave in lead V6).
With the above as background “static” changes (and without a prior tracing for comparison) — it’s obvious that this 85-year old at the least has extensive underlying coronary disease.
- Without a prior tracing for comparison — and without a much better appreciation of this patient’s symptoms and correlation between the presence and severity of chest pain at the time that this initial ECG was recorded — I found it hard to distinguish between “new” vs “old” vs “new superimposed on old”.
= = =
The Clues to Acuity …
The above said — I agree with Hans Helseth’s suspicion of an acute evolving event, although I would not activate the cath on the sole basis of ECG #1 without: i) More clinical information; — ii) Ideally finding a previous tracing on this patient (obviously an impossibility during helicopter transport of this patient to the hospital); — and, iii) Repeating the ECG (ideally within 10-20 minutes after the recording of this initial ECG). Nevertheless — there are clues to potential acuity in this tracing.
- Normally with uncomplicated RBBB — there is at least slight downsloping ST-T wave depression in lead V1. Instead, in lead V1 — there is ST segment coving, with an isoelectric (if not ever-so-slightly elevated) ST segment.
- Neighboring leads V2,V3 — demonstrate ST segment straightening with slight ST depression.
- This ST segment straightening with slight ST depression continues in leads V4,V5,V6.
- In the limb leads — there is fairly deep T wave inversion in leads III and aVF — with terminal T wave positivity in lead aVF (ie, potential indication of reperfusion T waves — as might be expected if there had been a recent OMI). ST segment straightening with depression is seen in lead II — with slight upsloping ST depression seen in high-lateral leads I and aVL.
- Finally — there is ST elevation in lead aVR — which in association with ST depression in multiple leads suggests DSI (Diffuse Subendocardial Ischemia), presumably from multi-vessel disease.
= = =
Figure-1: I’ve labeled the first 2 ECGs in today’s case.
= = =
The Repeat ECG …
As per Hans Helseth — the repeat ECG shows: i) LA-RA Lead Reversal (See Addendum below); — and, ii) Compared to ECG #1 — ECG #2 now clearly shows “dynamic” ST-T wave changes that confirm an acute OMI, and the need for prompt cath.
- Figure-1 emphasizes how much easier it is to compare serial ECGs — when you put both tracings side-by-side. Doing so, there can be no doubt that there is now a very deep negative component (a deep S wave that follows a tiny initial r wave) in lead I of ECG #2 (within the dotted RED rectangle) — that is associated with a deep negative T wave in this lead. These findings were not present in lead I of ECG #1.
- PEARL #1: You will almost never normally see this deep of a negative deflection prior to a positive R wave in left-sided lead I (especially when the P wave and T wave in this lead are also both negative — as they are in ECG #2). So, when you see the “picture” in lead I that we see within the dotted RED rectangle — Think RA-LA lead reversal.
NOTE: Hans Helseth showed in his discussion above — that correcting for the LA-RA lead reversal in ECG #2 confirmed that there had been “dynamic” ST-T wave changes consistent with acute infero-postero OMI.
- PEARL #2: The ST-T wave of a PVC may sometimes suggest an acute OMI — if this PVC displays ST-T wave changes “that clearly should not be there”. We see this phenomenon for the PVC in ECG #2 (the 2nd beat in simultaneously-recorded leads V1,V2,V3) — in which the RED arrow highlights a disproportionately increased amount of ST depression.
= = =
Addendum:
Lead reversals are surprisingly common — yet they still all-too-often pass unnoticed (Go To this LINK — for a list of lead reversals that have appeared on the pages of this ECG Blog).
- My favorite on-line “Quick GO-TO” reference for the most common types of lead reversal comes from LITFL ( = Life-In-The-Fast-Lane). I have used the superb web page they post in their web site on this subject for years. It’s EASY to find — Simply put in, “LITFL Lead Reversal” in the Search bar — and the link comes up instantly.
- This LITFL web page describes the 7 most common lead reversals. There are other possibilities (ie, in which there may be misplacement of multiple leads) — but these are less common and more difficult to predict.
- By far (!) — the most common lead reversal is mix-up of the LA (Left Arm) and RA (Right Arm) electrodes. This is the mix-up that occurred in ECG #2 of my Figure-1.
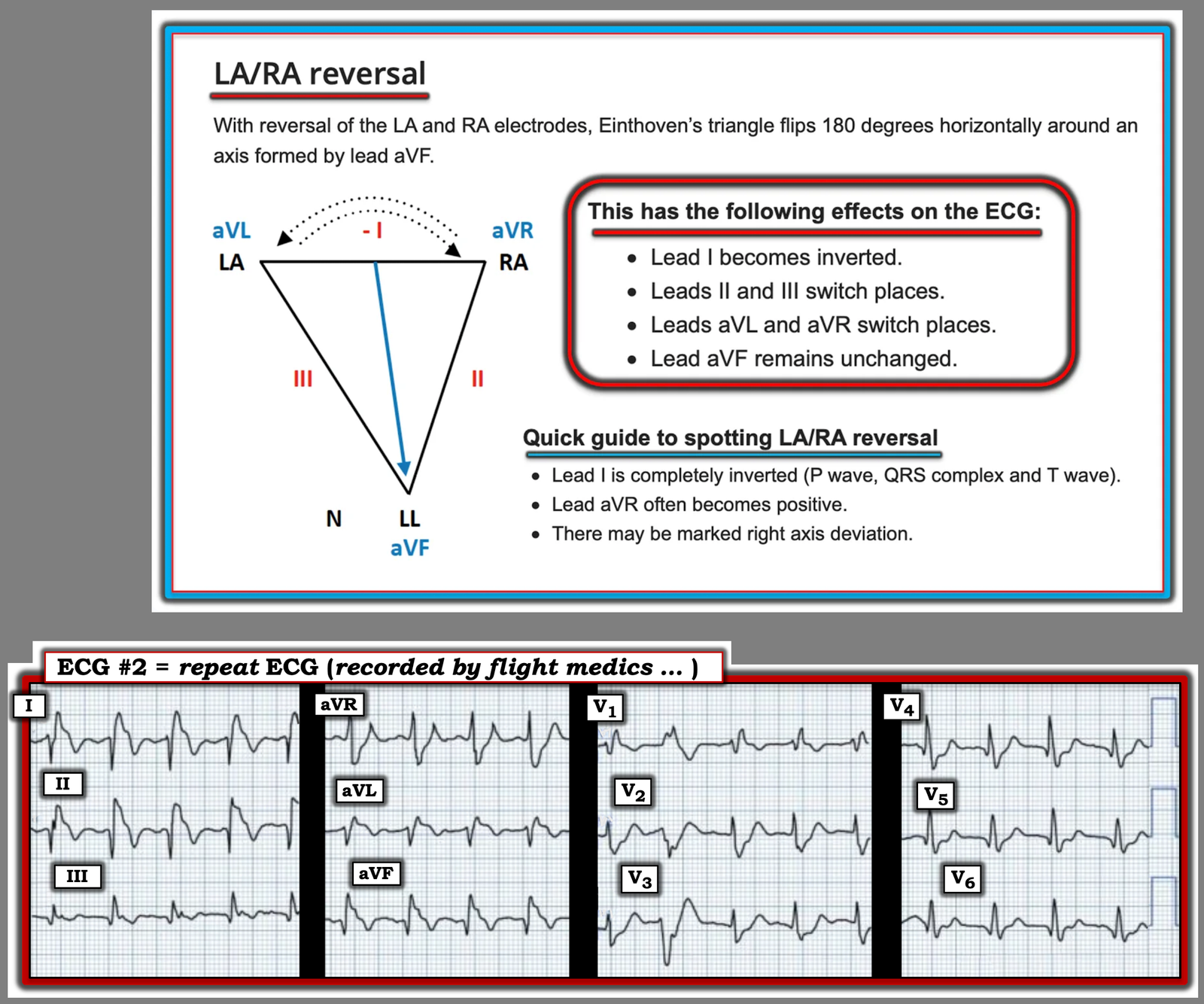
- For clarity in Figure-2 — I’ve reproduced the illustration from LITFL on LA-RA reversal — with today’s 2nd tracing below this. This should facilitate recognizing that there is indeed RA-LA lead reversal in ECG #2.
= = =
Figure-2 Effect on the ECG of LA-RA Lead Reversal (adapted from LITFL) — with the 2nd tracing in today’s case below.
= = =
===