I saw this patient in triage.
“47 y.o. male presents for syncope today. States he passed out while standing, first feeling dizzy and nauseous then losing consciousness for a few seconds. He went down slow and he did not strike his head. No chest pains, abdominal pain, vomiting, or headaches. States he feels shaky.”
He is very healthy, with no past history, no medications, feels well now. see history below.
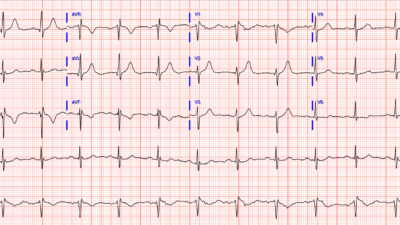
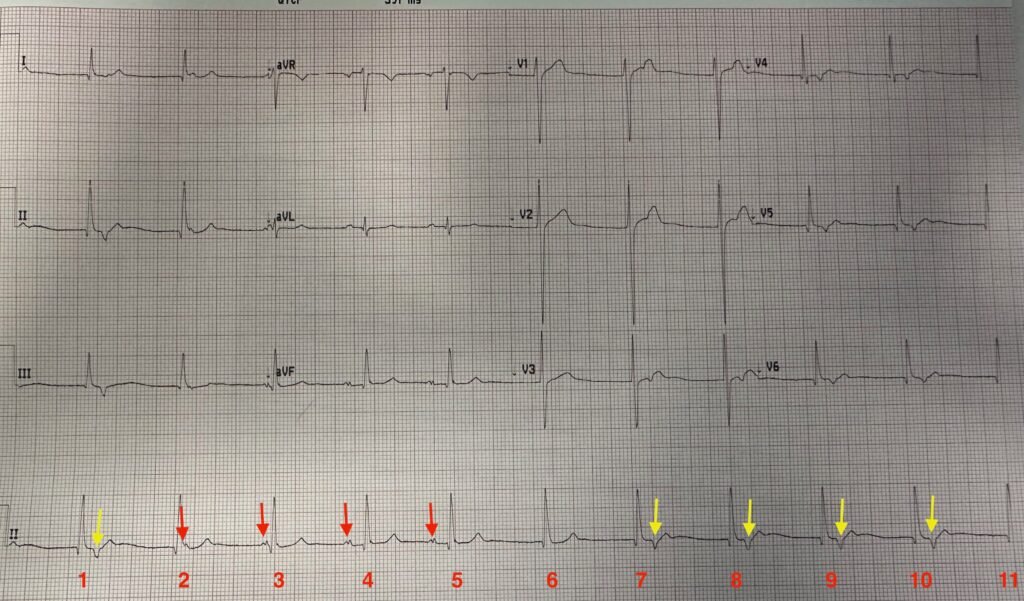
We recorded this ECG:

What is the Rhythm?
I thought immediately that it shows an accelerated junction rhythm, with some retrograde P-waves, and thus is “Isorhythmic Dissociation”, which is a safe rhythm. Isorhythmic dissociation can be either due to either:
1. “default” — this is due to sinus node slowing — the AV node escapes because it is the default rhythm when the sinus node is not firing, or
2. “usurpation” — this is when the AV node accelerates and “usurps” the sinus node.
This case ECGs shows a COMBINATION of both “default” and “usurpation”
Electrolytes were normal and troponin undetectable.
I was convinced this was vasovagal syncope and discharged the patient from triage.
Below is Ken Grauer’s more detailed analysis, using this nice graphic and a laddergram:
MY Comment, by KEN GRAUER, MD (6/9/2025):
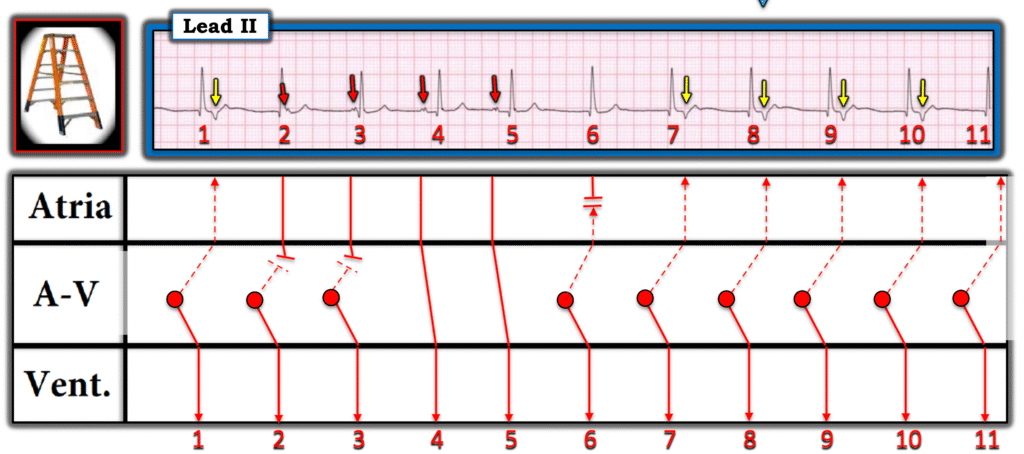
The above laddergram suggests my thoughts on the rhythm mechanism:
- Overall, the rate of sinus P waves ( = the rate of the 4 RED arrows) is not that slow — it is actually ~70/minute.
- There is AV dissociation for the first 2 RED arrows — but presumably sinus conduction for beats #4 and 5 (since the PR interval is the same for these 2 beats). In support of sinus conduction for beats #4 and 5 — is the fact that beat #5 occurs a little earlier-than-expected while maintaining the same PR interval that precedes beat #4 (Technically I’d need to see more monitoring with additional sinus-conducted beats showing this same PR interval to be certain about sinus conduction).
- The sinus P wave rate then presumably slows after beat #5 — which is why we do not see any P wave before beat #6.
- NOTE: How much the sinus P wave rate slows after beat #5 is uncertain — because beat #6 is a slightly accelerated junctional beat (with a preceding R-R interval just less than 5 large boxes ==> which corresponds to a slightly accelerated junctional escape rate of ~65/minute).
- Following junctional beat #6 — We begin to see retrograde P waves after junctional beats #7,8,9 and 10 (YELLOW arrows — that manifest a surprisingly long but constant RP’ interval).
- NOTE: The junctional escape rate is slightly accelerated to ~67/minute for beats #7-thru-11 — so presumably the reason we are not seeing any more sinus P waves after beat #5 is because the SA node has slowed below 67/minute (but not necessarily a lot below that — as the retrograde P waves might prevent the SA node from “waking back up”).
Bottom Line: I would describe the rhythm in Figure-1 as sinus arrhythmia with intermittent AV dissociation due to a combination “default” (from intermittent sinus slowing) and “usurpation” (from the slightly accelerated junctional pacemaker).
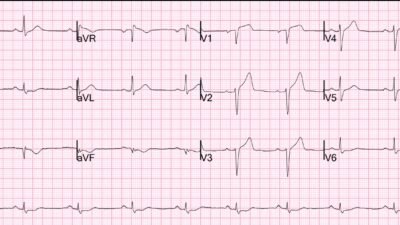
- The 12-lead ECG does not show any acute changes — so the rhythm in Figure-1 is not necessarily pathologic. An increase in vagal tone (from whatever reason) might account for this. Although we usually do not see retrograde P waves with junctional beats — this is not necessarily pathologic.
- Perhaps the reason for the syncopal episode (and for the rhythm in Figure-1) in this otherwise healthy person is simply the result of a temporary increase in vagal tone?
- Depending on specifics of the history and physical exam — all that may be needed might be consideration of the usual reasons for syncope (prescribed or illicit drug use, alcohol, dehydration, orthostatic hypotension, etc.) — and some limited period of cardiac monitoring to ensure there is no excessive slowing of the overall heart rate.
= = =
NOTE: For more on “usurpation” and “default” as potential causes of AV dissociation (as well as how to distinguish between AV Dissociaton vs Complete AV Block) — Check out my 5-minute ECG Video on this subject!
- CLICK HERE — for my 5-minute ECG Video on Laddergram Basics (with step-by-step illustrations and LINKS to all laddergrams that I have drawn in Dr. Smith’s ECG Blog).
= = =
= = =