By Jesse McLaren
A previously healthy 65 year old male presented with one hour of sudden, severe, non-radiating mid abdominal pain with nausea and diaphoresis. BP was 190/100, HR 60, normal respiration and oxygen saturation.
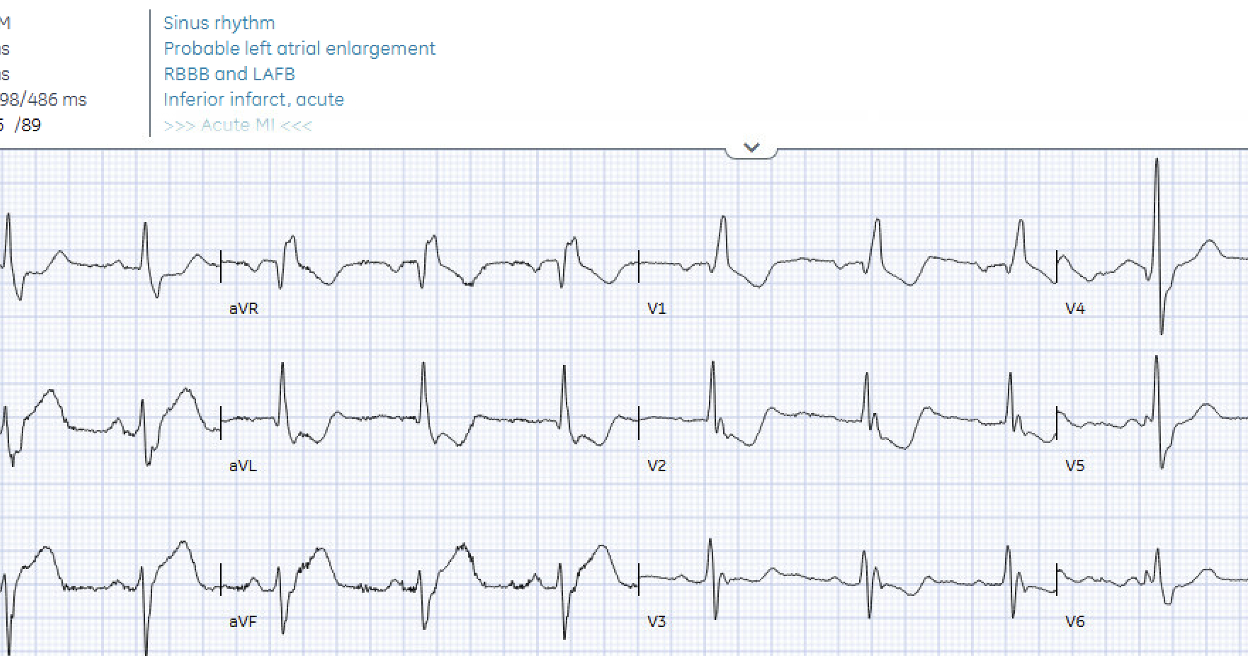
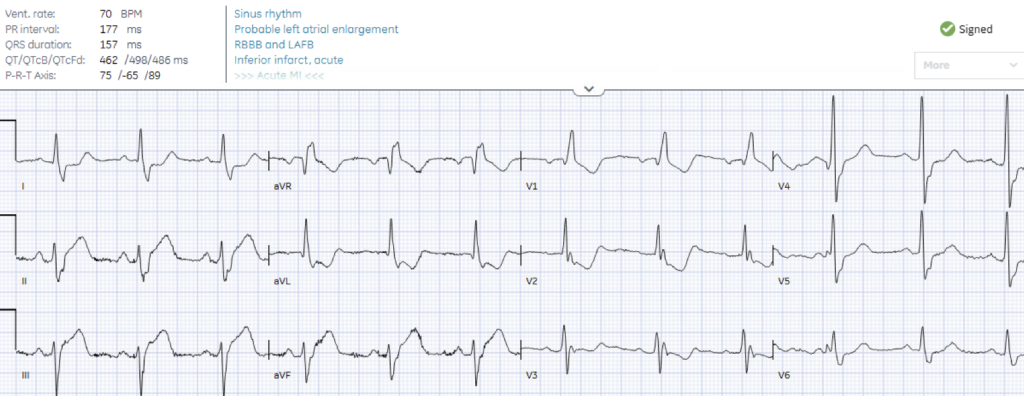
The final ECG interpretation by the blinded cardiologist was acute inferior MI, but the patient had no chest pain. What do you think?
What do you think?
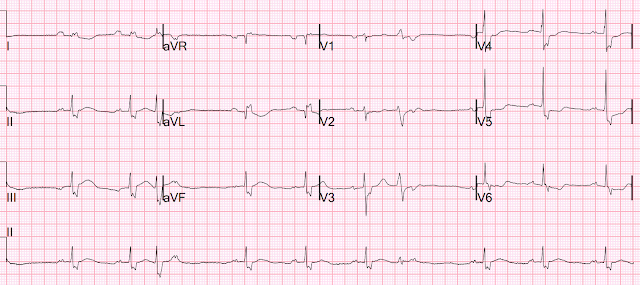
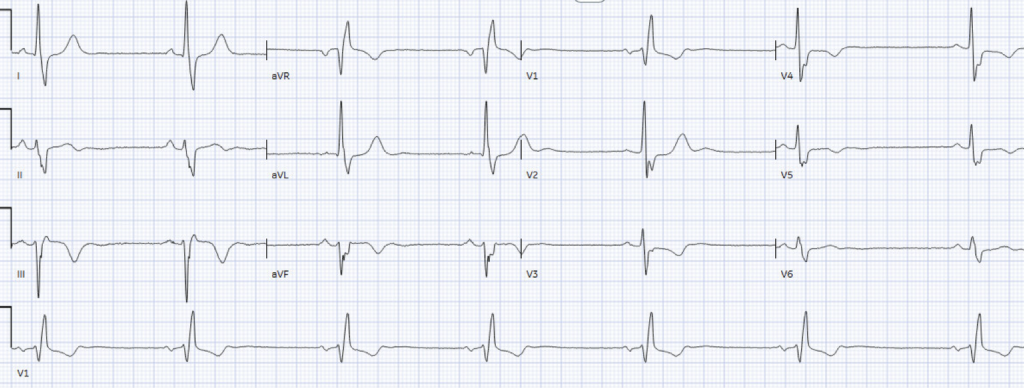
There’s normal sinus rhythm, RBBB and LAFB, and normal voltages. There’s inferior ST elevation that meets STEMI criteria, along with hyperacute T waves with reciprocal ST Depression and T-wave inversion in aVL (inferior OMI), and excessively discordant STD/TWI in V2 (posterior OMI). RBBB/LAFB can be an acute complication of proximal LAD occlusion, but infero-posterior OMI is usually caused by RCA occlusion that does not affect the right bundle or left fascicles. (Smith: there probably was a pre-existing RBBB/LAFB)
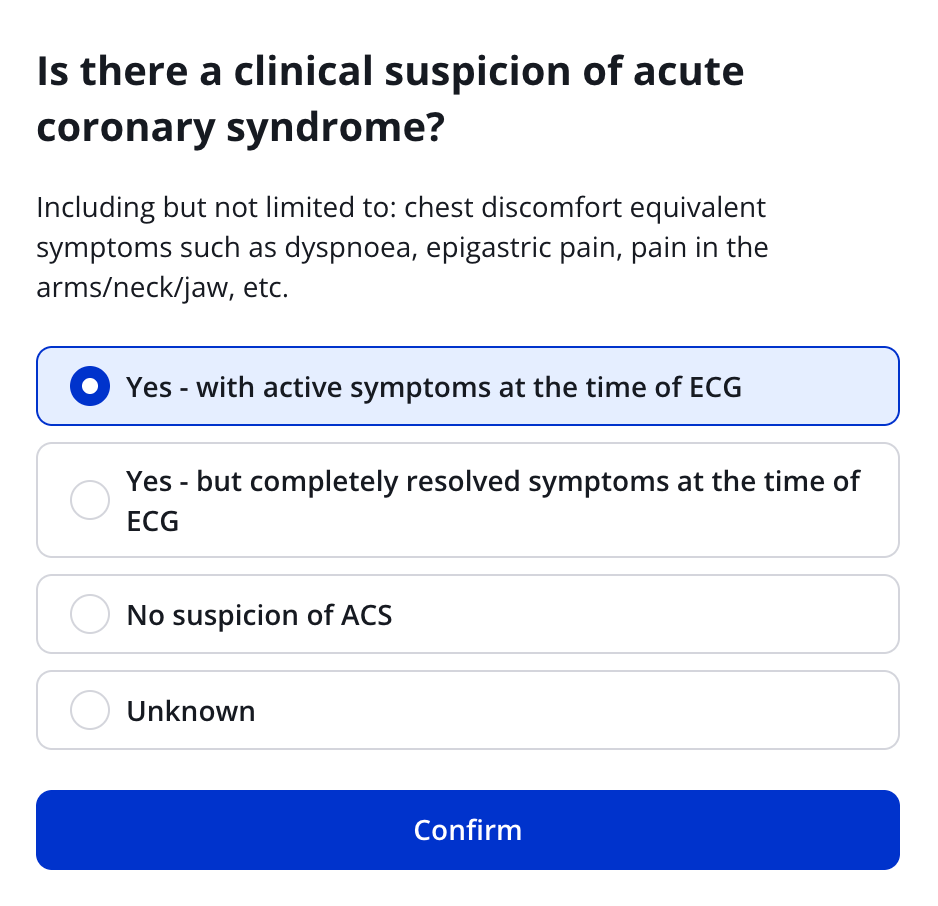
So the ECG had a blinded interpretation of inferior STEMI. The Queen of Hearts also interprets ECG blinded to clinical context but with the initial question of whether the patient has active ACS symptoms, resolved ACS symptoms, or no concerns for ACS.
Here is how the Queen asks this question:
If you tell the Queen there was no concern for ACS, she still highlights the diagnostic changes of infero-posterior OMI (without the need for posterior leads), but cautions to interpret in clinical context.
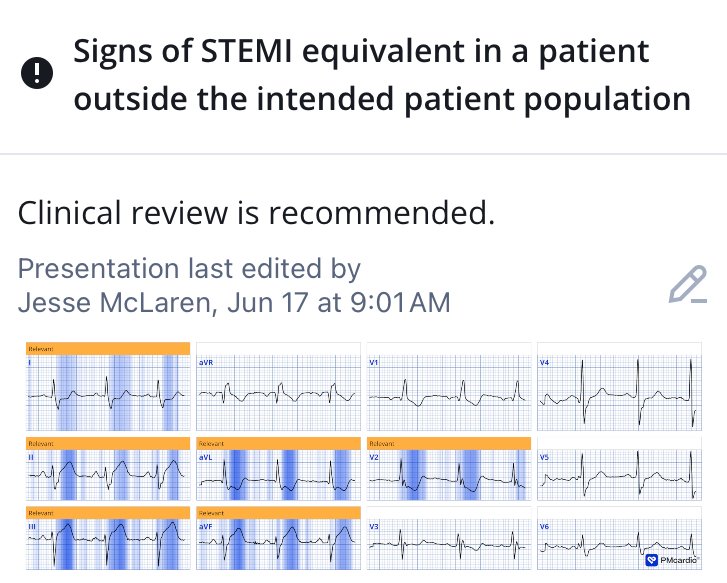
The Queen of Hearts sees BOTH inferior and posterior OMI (STEMI or STEMI equivalent).
_______
Smith: Anyone with abdominal pain and diaphoresis has a suspicion of ACS, which Jesse explains in detail below. Notice that the Queen asks: “Including but not limited to: chest discomfort equivalent symptoms such as dyspnoea, epigastric pain, pain in the arms/neck/jaw, etc.” Although acute MI can present silently, this is NOT silent. This patient is symptomatic.
Here is a case of a truly silent acute MI.
And another: Should Troponin be a Vital Sign? Perhaps, but only if Interpreted Using Pre-test Probability.
Here is the Queen’s interpretation if you answer in the affirmative about symptoms:

Case Continued:
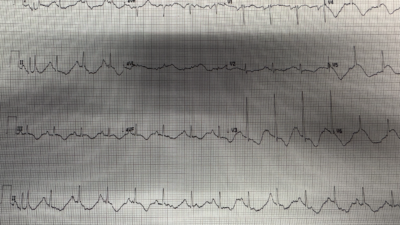
The emergency physician noted the inferior STE and reciprocal change in aVL on ECG. On exam the abdomen was soft, with tenderness above the umbilicus without guarding, and POCUS found no AAA or cholecystitis to explain the pain. The patient was given analgesia (for symptom control, not as a diagnostic tool) and a 15-lead ECG was done 20 minutes after the first:

There is still infero-posterior OMI (with false negative posterior leads), as well as STE in V4R (Smith: this is all but diagnostic of RV infarct due to proximal RCA occlusion. This should heighten your suspicion even more). So the patient was given nitro spray and cardiology consulted stat for possible STEMI in the absence of chest pain.
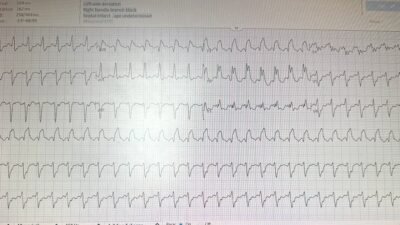
Cardiology did not think the history was compatible with STEMI. They noted epigastric pain and tenderness, POCUS was inconclusive for wall motion abnormalities (Smith: POCUS is not sensitive for wall motion abnormalities, especially since bubble contrast is not used), and initial high sensitivity troponin I was 8ng/L which is normal (<16 in females and <26). So the patient had a CT chest/abdo/pelvis for aortic dissection or abdominal causes, which was normal. Serial troponin over the next few hours was 16 (still normal) and then 180 ng/L. The patient had ongoing epigastric pain and developed bradycardia, with a change in the ECG:
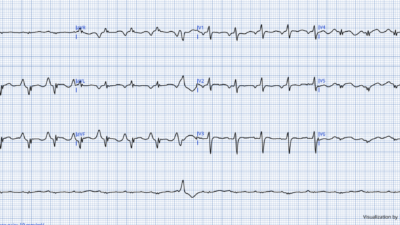
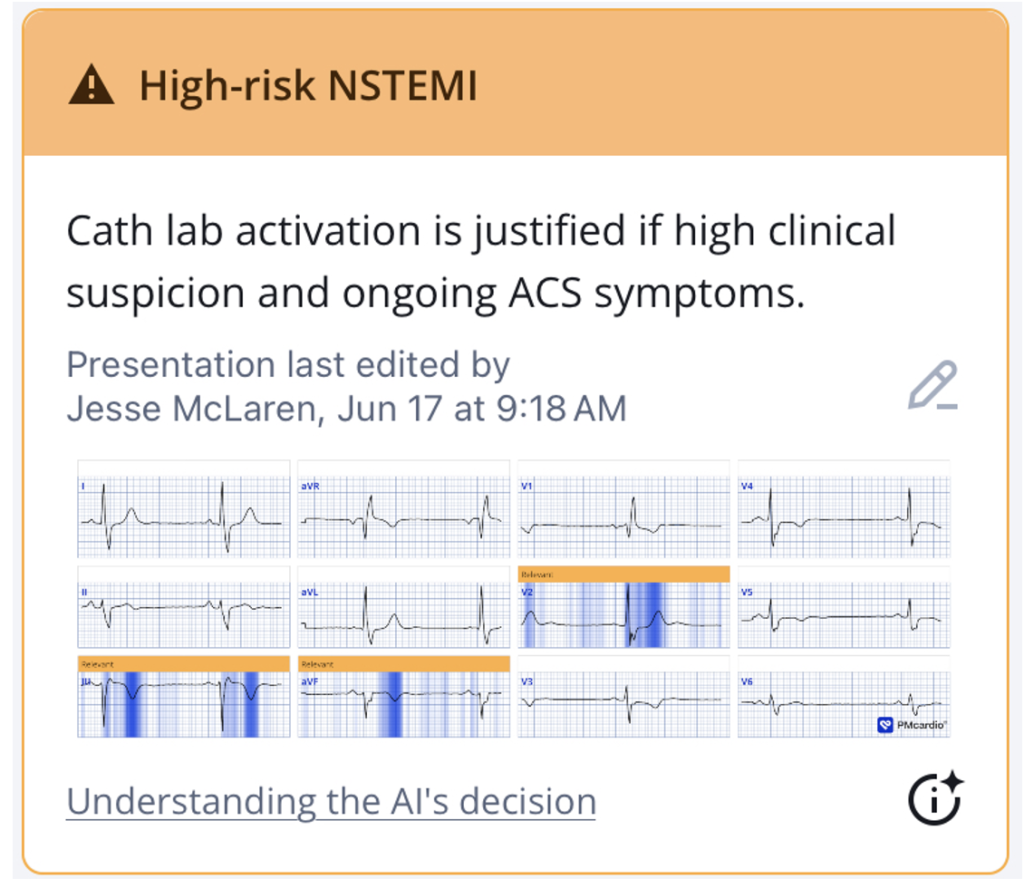
There is sinus bradycardia, the ST segment changes have resolved and the hyperacute T waves had deflated and inverted (with reciprocally tall T wave in V2). This suggests reperfusion, but the patient still had epigastric pain. The Queen highlights the reperfusion changes on ECG, but advises cath lab activation if high clinical suspicion and ongoing ACS symptoms:
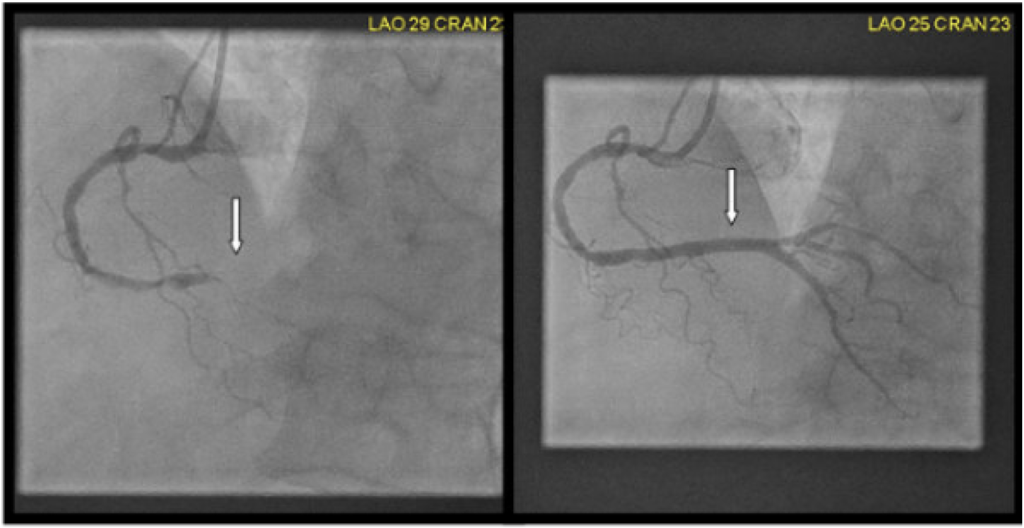
With ongoing epigastric pain, dynamic ECG changes and transient bradycardia, and a rising troponin with other causes excluded, the cath lab was activated. Door to cath time was 6 hours and angiogram showed a 100% mid RCA occlusion. Below are pre and post-stent angiography images:
EF was reduced to 44% with inferior akinesis and hypokinetic basal to distal inferolateral wall, and there was a massive peak troponin of 100,000 ng/L (a good measure of very large infarct size).
ACS ≠ Acute Chest pain + STE
ACS has been equated with acute chest pain + ST elevation. But 1) most ED patients with chest pain do not have ACS, 2) many acute MI present without chest pain, 3) most ED patients with chest pain and STE do not have MI, and 4) most OMI present without STE.
- A new national study in the US of ED patients with a chief complaint of atraumatic chest pain found that 5.5% (and 9.4%>64 years) were diagnosed with one of 7 life-threatening conditions (ACS, PE, pneumothorax, aortic dissection, Boerhaave, tamponade, ruptured AAA). The most common diagnosis was ACS at 4.5% (vs 0.09% for aortic dissection). But most of these diagnoses presented without chest pain as a chief complaint, including ACS (47%). So the overall pre-test likelihood for ACS in ED patients with chest pain is low, but lack of chest pain does not exclude ACS. By focusing on chief complaint this study likely underestimated the occurence of chest pain, for example with patients presenting with a chief complaint of shortness of breath or epigastric pain who on further history also had chest pain. Chest pain/pressure is a typical ACS symptom, but so are anginal equivalents such as shortness of breath or epigastric pain, and lack of chest pain does not exclude ACS or predict a more benign course.
- On the contrary, ACS without chest pain is a bad prognostic factor. Studies have consistently shown that ACS without chest pain is a common presentation, especially in older, female patients and those with comorbidities, and that it leads to delayed diagnosis/treatment and higher mortality rates. [like here (Brieger et al.), here (El Menyar et al.), here (Bjork et al.) and here (Pong et al.)]
- See references below.
- Canto et al. published this very large study in JAMA in year 2000 and found that 1/3 of STEMI and 1/3 of NSTEMI present without chest pain.
Canto JG, Shlipak MG, Roger WJ. Prevalence, clinical characteristics, and mortality among patients with myocardial infarction presenting without chest pain. JAMA 2000;283(24):3223–9.- Results Of 434,877 patients from 1674 hospitals who were diagnosed as having MI, 142,445 (33%) did not have chest pain on presentation to the hospital. This group of MI patients was, on average, 7 years older than those with chest pain (74.2 vs 66.9 years), with a higher proportion of women (49.0% vs 38.0%) and patients with diabetes mellitus (32.6% vs 25.4%) or prior heart failure (26.4% vs 12.3%). Also, MI patients without chest pain had a longer delay before hospital presentation (mean, 7.9 vs 5.3 hours), were less likely to be diagnosed as having confirmed MI at the time of admission (22.2% vs 50.3%), and were less likely to receive thrombolysis or primary angioplasty (25.3% vs 74.0%), aspirin (60.4% vs 84.5%), β-blockers (28.0% vs 48.0%), or heparin (53.4% vs 83.2%). Myocardial infarction patients without chest pain had a 23.3% in-hospital mortality rate compared with 9.3% among patients with chest pain (adjusted odds ratio for mortality, 2.21 [95% confidence interval, 2.17-2.26]).
- This is compounded by the poor sensitivity and specificity of STE for acute coronary occlusion. Most ED patients with ST elevation do not have MI, but have STE secondary to LBBB/LVH or proportional to tall voltages with normal variant/early repolarization. These lead to false positive activations.
- And most patients with Occlusion MI present without STEMI criteria, leading to delayed reperfusion and higher mortality rates (shown here and here). The QOH can identify both false positive STEMI and subtle occlusions.
- Epigastric pain without chest pain was the presenting symptom in up to 11% of anterior MI and 16% of inferior MI in this study by Culic et al.
Therefore a Bayesian approach to OMI is needed (described here and with cases here): pre-test likelihood (including anginal equivalents, refractory ischemia and electrical instability) + test (ECG signs of OMI, POCUS for regional wall motion abnormalities, +/- troponin), guiding post-test management.
With high pre-test likelihood, subtle ECG signs of OMI can help expedite angiography. With very high pre-test likelihood (eg refractory ischemia with hemodynamic instability and regional wall motion abnormality), the ECG is not needed. In this case the test showed clear STEMI, but the pre-test likelihood was deemed so low because of the absence of chest pain, reinforced by the physical exam and initial troponin test. But lack of chest pain is common in MI, reproducible tenderness is commonly found in patients with MI, and a troponin after only one hour of symptoms is not helpful. While the overall pre-test likelihood of ACS in the ED is low, lack of chest pain does not exclude it, and a STEMI(+)OMI ECG greatly raises post-test likelihood for OMI. Aortic dissection has a far lower pre-test likelihood, and if there is STEMI on ECG, the likelihood of this being secondary to aortic dissection is 0.5%. In the absence of POCUS signs of dissection, CT scan will delay reperfusion for OMI in the vast majority of cases.
Fortunately, the cath lab was eventually activated despite resolution of STE based on clinical signs of OMI (refractory ischemia and transient bradycardia), and rising troponin.
Take away
- Lack of chest pain does not exclude STEMI/Occlusion MI, and ACS without chest pain is associated with delayed treatment and higher mortality.
- The first troponin after an hour of symptoms is not helpful, and the initial troponin rise does not predict its peak.
- STEMI secondary to aortic dissection is very rare.
- Reperfusion requires both symptomatic and ECG resolution.
- Queen of Hearts can identify occlusion and reperfusion, both of which require clinical correlation.
Even when an ECG is BOTH Diagnostic of OMI AND meets STEMI criteria, patients often receive negligent care. This is malpractice.
Selected references:
Brieger D, Eagle KA, Goodman SG, et al. Acute coronary syndromes without chest pain, an underdiagnosed and undertreated high-risk group: insights from the Global Registry of Acute Coronary Events. Chest [Internet] 2004;126(2):461–9. Available from: http://dx.doi.org/10.1378/chest.126.2.461
El-Menyar A, Zubaid M, Sulaiman K, et al. Atypical presentation of acute coronary syndrome: a significant independent predictor of in-hospital mortality. J Cardiol [Internet] 2011;57(2):165–71. Available from: http://dx.doi.org/10.1016/j.jjcc.2010.11.008
Björck L, Nielsen S, Jernberg T, Zverkova-Sandström T, Giang KW, Rosengren A. Absence of chest pain and long-term mortality in patients with acute myocardial infarction. Open Heart [Internet] 2018;5(2):e000909. Available from: http://dx.doi.org/10.1136/openhrt-2018-000909
Pong JZ, Ho AFW, Tan TXZ, et al. ST-segment elevation myocardial infarction with non-chest pain presentation at the Emergency Department: Insights from the Singapore Myocardial Infarction Registry. Intern Emerg Med [Internet] 2019;14(6):989–97. Available from: http://dx.doi.org/10.1007/s11739-019-02122-3
= = =
==================================
MY Comment, by KEN GRAUER, MD (6/26/2026):
In the title of today’s post by Dr. McLaren — He asks the question, “Does the lack of CP (Chest Pain) exclude STEMI/OMI?”. The answer to this question is a resounding NO!
- FACT #1: Although CP is by far the most common symptom experienced with acute MI — atypical presentations (ie, with pain or discomfort in other body areas) as well as acute MI without CP or any other symptom at all, continue to occur much more commonly than is commonly appreciated (Khan et al: Cureus 15(2):e35492, 2023 — and — Björck et al: Open Heart 5:e000909, 2018).
- FACT #2: As per Dr. McLaren (and as we have repeated shown in cases presented in Dr. Smith’s ECG Blog) — the initial Troponin (and sometimes even a 2nd Troponin) may be negative despite the presence of an ongoing acute infarction.
- Clinical Reality: Until the above 2 facts become accepted by emergency care providers (including the Cardiologist in today’s case, who refused to accept these facts) — acute OMIs, and even STEMIs will continue to be overlooked to the detriment of patient care.
= = =
The first 2 ECGs …
The entity we call, “Fake” clearly exists (in which an ECG may look like an acute infarction — but turns out not to be an infarction). That said — the tough lesson that hopefully is learned from today’s case, is that even when the initial Troponin is normal and the patient does not have CP — IF the initial ECG “looks like” an acute MI, this ECG must be believed until we prove otherwise.
- For clarity in Figure-1 — I’ve reproduced and labeled the first 2 ECGs in today’s case.
- PEARL: Putting these first 2 tracings together in the same figure facilitates recognition of subtle-but-present “dynamic” ST-T wave changes.
= = =
Take another LOOK …
- Do YOU see these subtle dynamic changes in Figure-1?
= = =
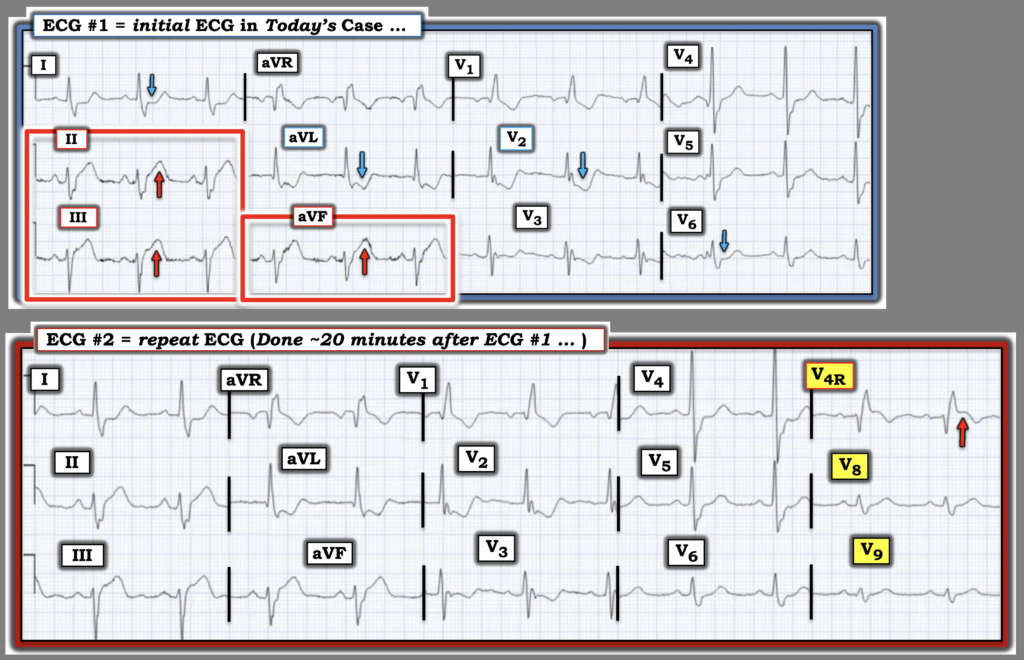
Figure-1: I’ve labeled the first 2 ECGs in today’s case.
= = =
Answer: The ECGs in Figure-1 ….
The initial ECG in today’s case shows sinus rhythm with multiple abnormal findings that for all the world look like an acute STEMI until proven otherwise (Witness interpretation as “an acute inferior MI” by the blinded cardiologist). As per Dr. McLaren — Among the abnormal ECG findings in ECG #1 are the following:
- Bifascicular block (RBBB/LAHB) of unknown age (ie, Without access to a previous ECG — we don’t know if this conduction defect is new or old).
- Hyperacute ST-T waves in each of the inferior leads (RED arrows highlighting taller and “fatter” T wave peaking with ST segment straightening, ≥2 mm J-point elevation, and a very much wider-than-expected T-wave base in leads II,III,aVF).
- Marked reciprocal ST-T wave depression in both lead aVL and lead I (BLUE arrows in these leads).
- Clearly more-than-expected ST-T wave depression in lead V2. With typical RBBB — the amount of ST-T wave depression in anterior leads is typically greatest in lead V1, with progressive reduction as one moves across the chest leads. In contrast — the BLUE arrow in lead V2 highlights an unanticipated marked increase in the J-point ST depression that we see in this lead. As per Dr. McClaren — this suggests acute posterior OMI until proven otherwise.
- Finally — there is subtle ST segment straightening with slight depression in lead V6.
Additional fine points to consider include the following:
- Note #1: As often emphasized in Dr. Smith’s ECG Blog — analgesia should not have been given after the 1st ECG was obtained, since no clinical diagnosis had yet been made.
- This is because if serial ECGs show improvement after analgesia — We will not know if this reflects reduction of symptoms because of spontaneous reperfusion or reduction of symptoms because of analgesia.
- Note #2: Twenty minutes passed after ECG #1 was recorded before a 2nd ECG with 15 leads was recorded. The reason I would have favored immediately recording the 15-lead ECG (instead of waiting 20 minutes) — is that we lose the ability to compare what additional leads V4R,V8,V9 looked like in the initial tracing.
- Clinically, this does not matter in ECG #2 for lead V4R — because the RED arrow in this lead highlights such obvious ST elevation from acute RV involvement.
- But it may account for the false negative leads V8,V9 that fail to show ST elevation from this patient’s acute posterior OMI (As shown in the September 21, 2022 post, among many others — posterior leads are not nearly as accurate as seeing maximal ST depression in leads V2,V3,V4 for assessing posterior OMI).
- Note #3: As often emphasized in Dr. Smith’s ECG Blog — Serial ECGs must be interpreted with lead-by-lead comparison of both tracings IF one hopes to avoid overlooking subtle changes.
- Isn’t there suggestion in Figure-1 of subtle-but-real improvement in the degree of hyperacuity seen in the inferior leads in ECG #2 compared to ECG #1?
- As a result — I interpreted these probable “dynamic” ECG changes that are seen in the repeat ECG done 20 minutes later (especially in view of the obvious ST elevation in lead V4R) — as evidence of ongoing acute infero–postero OMI until proven otherwise regardless of the normal initial Troponin and absence of CP.
= = =
BOTTOM Line: An ECG that “looks like” an acute MI could be a “fake” (ie, Pseudo-infarction pattern) — but we need to minimize delay in proving that this ECG is not an acute MI, especially when the patient presents with a new acute symptom (such as the sudden onset of severe abdominal pain).
- Neither a normal initial Troponin nor the absence of CP constitute sufficient “proof” — as was clearly shown in today’s case.
= = =
= = =