This was sent by Jack Cahill, a medical student in Britain who is a young ECG savant (like Hans Helseth).
This 20-something patient collapsed into a cardiac arrest whilst playing football, without a reported/declared prodrome.
He was found in ventricular fibrillation, requiring cardiopulmonary resuscitation and five defibrillating shocks to achieve a return of spontaneous circulation, around 20 minutes after collapse.
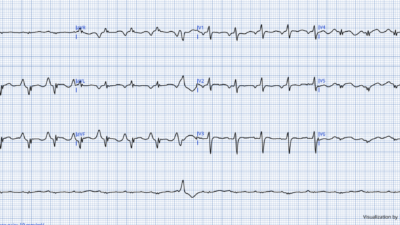
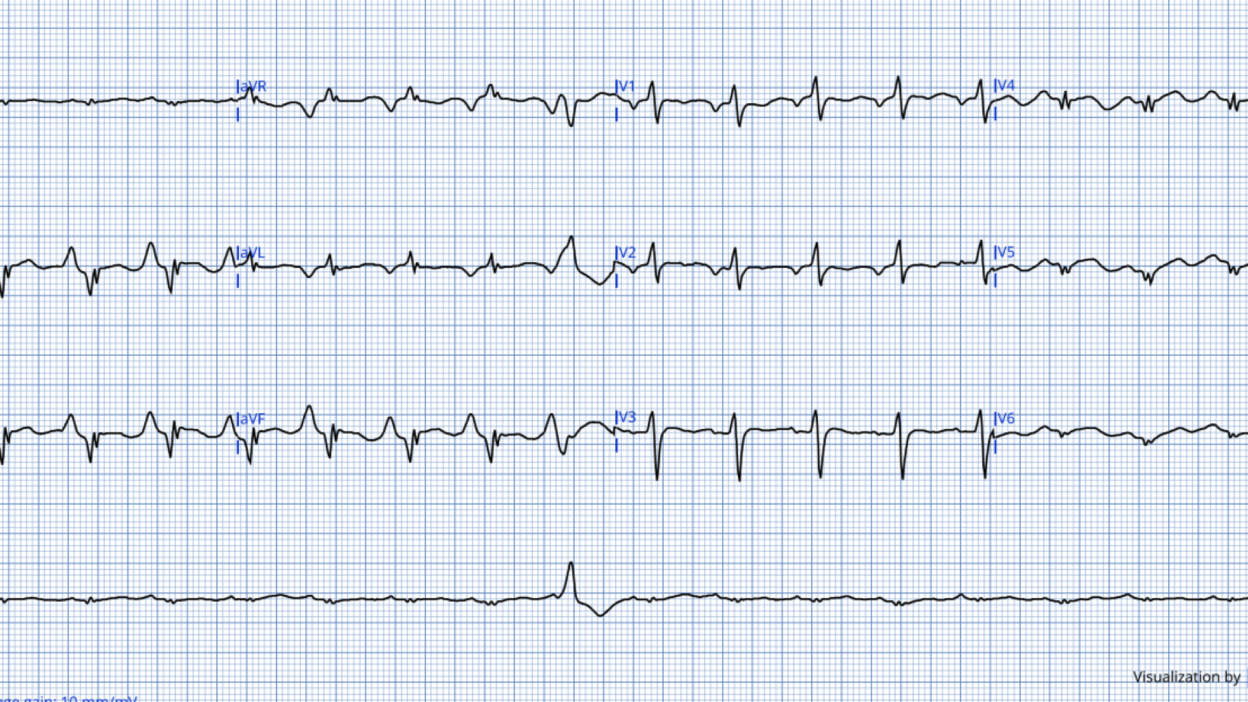
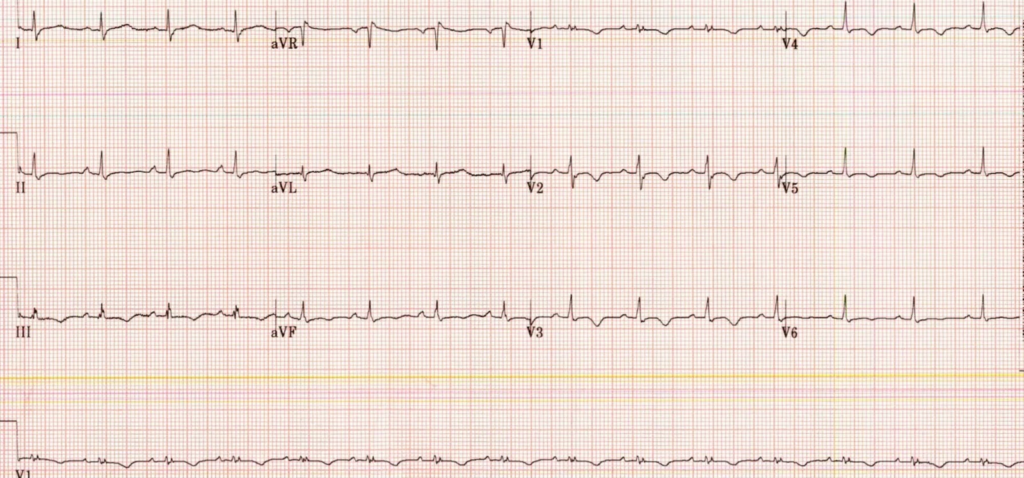
This was his post-ROSC ECG (~20 mins later):
What do you think? Does the patient need the cath lab?
This is a grossly ‘pulmonic ECG’; There is P-pulmonale, Reduced voltage, Dominant R in V1 with T-wave inversion (though shallow) in V1-4. There is also “Schamroths Sign” in Lead I (very low voltage usually due to vertical heart in COPD resulting in vertical QRS axis, which leaves lead I with very low voltage — sensitivity and specificity unknown)
There are also Qr complexes in the inferolateral leads with enlarged ST-Ts. One must always consider acute ischaemia, irrespective of the patient’s age. VF cardiac arrest is most commonly caused by ischaemia. It would not be wrong to take this person to the Cath lab. The T waves are hyperacute in V4 and V5 – mimicking an infarction pattern.
It is very likely that there are a multitude of factors contributing to this trace, including cardiogenic shock, post-arrest myocardial stunning, with reduced contractility and stroke volume, possible right ventricular failure and other mechanical causes of impaired forward flow, superimposed on underlying structural cardiac pathology.
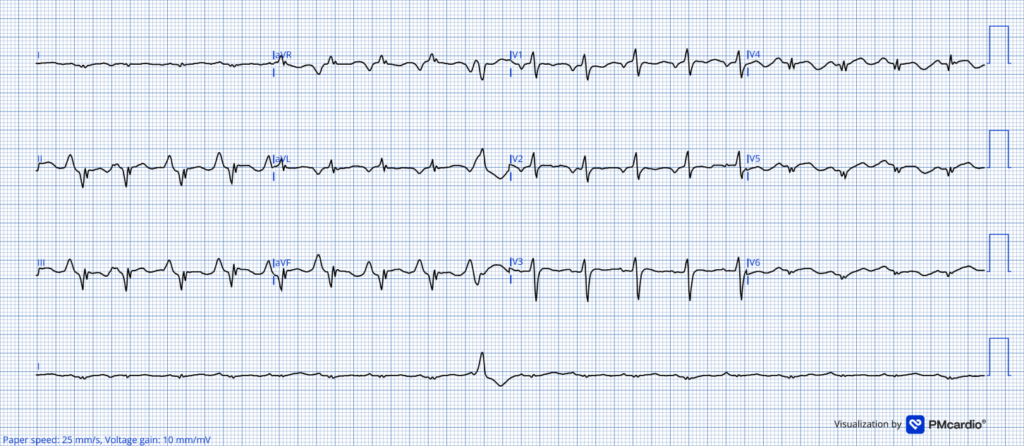
The Queen, however, recognises this is not OMI:
Notice that she also thinks that the LVEF is < 40%
The patient was transferred to ICU for post-cardiac arrest care, where he was intubated and ventilated and managed with neuroprotective measures. He required 0.29 mcg/kg/min Noradrenaline to maintain an invasive arterial pressure ~75/60 mmHg (MAP~65mmHg), producing a narrow pulse pressure, consistent with post-arrest myocardial stunning superimposed on possible underlying cardiomyopathy / ventricular dysfunction. CT head was also unremarkable.
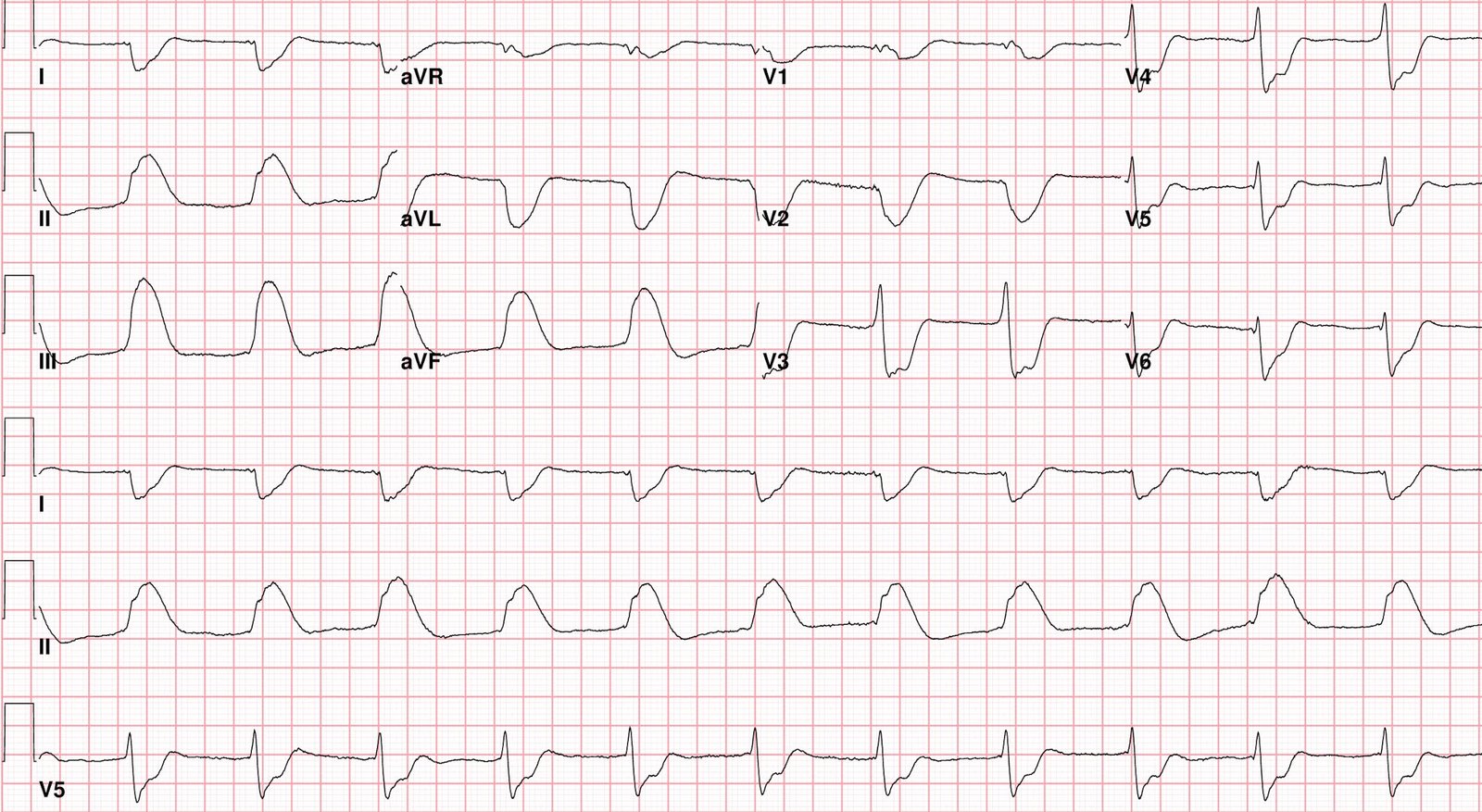
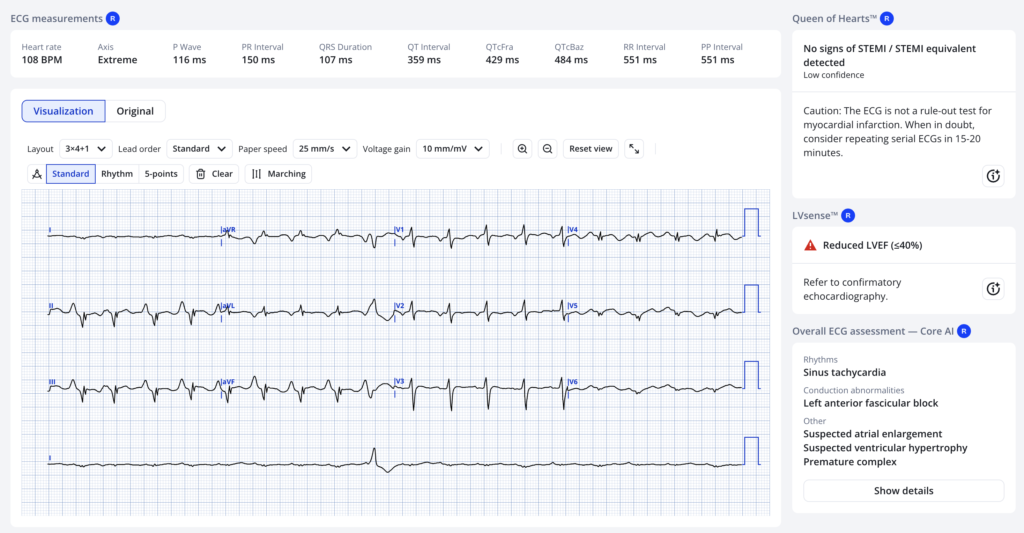
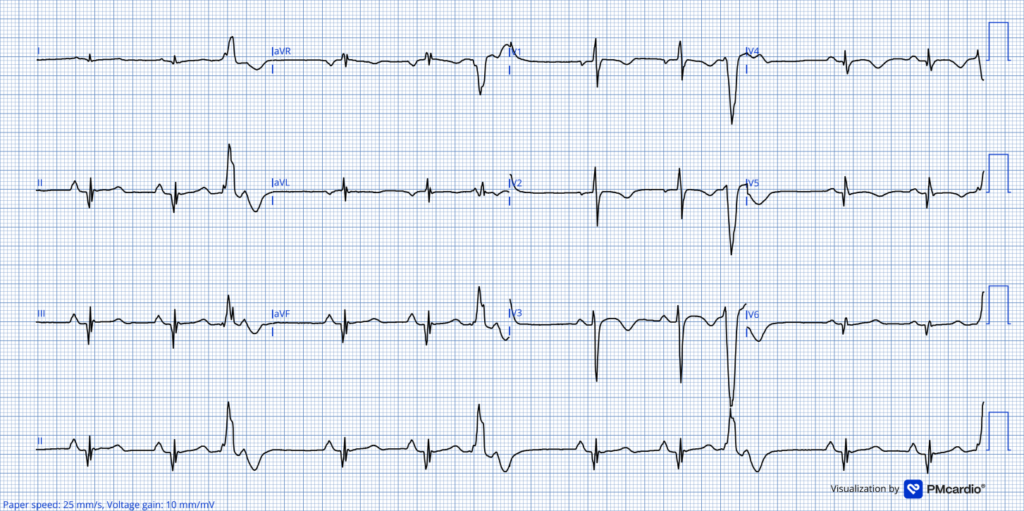
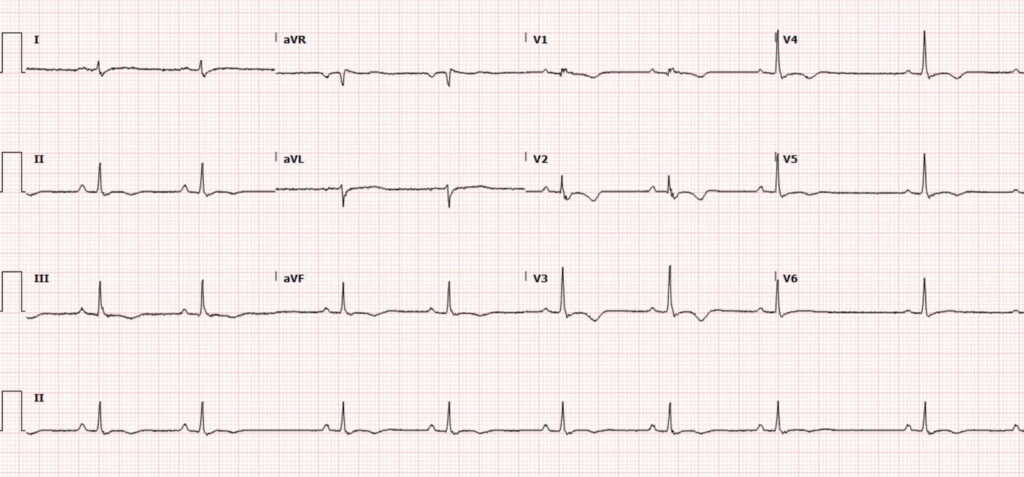
This was the ECG, whilst on ICU:
There is sinus rhythm with a PR ~170ms, QRS ~105ms, QRS axis ~-65, QTc ~ 440ms.
There is again very low voltage in Lead I (Schamroths Sign), likely due to a vertical/rightward shift in the QRS axis.
P-Pulmonale – Enlarged P amplitude in Lead II, suggesting possible right atrial enlargement or pressure overload.
A dominant R in V1, with reverse R wave progression across the precordium, transitioning from an Rs morphology to a Qr complex. This indicates significant abnormal ventricular activation and is suggestive of structural right ventricular pathology with possible biventricular involvement.
T wave inversion is present in V1-3 is very consistent with RV pathology, but the T-wave inversion in V4-5 could be either RV or a sign of reperfusion. Large, pathological Q waves in Leads II, III, aVF, V4-6 are also seen. Likely reflecting abnormal right ventricular depolarisation-repolarisation associated with underlying dominant-right ventricular structural disease but raising the possibility of both RV and LV involvement.
The Queen also sees possible reperfusion:

Frequent premature ventricular contractions (PVCs) are present, which have a predominantly negative configuration in V1-3 (rS morphology), suggesting the PVCs are likely spreading from right to left (away from V1). The complexes are positive in leads II and III, suggesting they are vectoring inferiorly. We are just capturing a late R-wave transition at the end of the strip, suggesting that together, these PVCs are from around the right ventricular outflow tract. It is probable that there is also retrograde ventriculoatrial activation, which is not uncommon. We see evidence of this during the R-T transition.
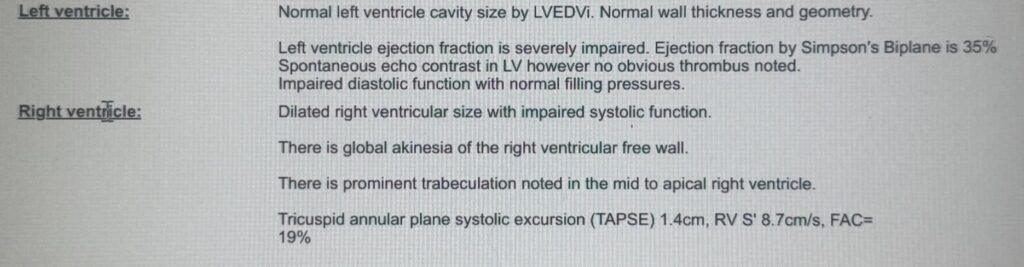
Here is the echo:
So…
- What is the most likely diagnosis?
- What is the most likely mechanism behind the cardiac arrest in this patient?
The patient was stepped down from ICU to an acute cardiac care unit, where he remained stable and was worked up for a subcutaneous ICD implantation.
Cardiac MRI confirmed a non-ischaemic cause for this patients’ arrest – summary:
Biventricular Dilatation and Systolic Dysfunction
Wide-spread Non-ischaemic biventricular scarring/fibrosis
LGE of the epicardium and mid-myocardium in the lateral, Inferoseptal, apical and RV-free wall, which was also akinetic
No evidence of inflammation, normal valves, atria and great arteries
Answers:
- Arrythmogenic Cardiomyopathy (ACM) (in this case, biventricular)
- See this post for lots of info on Arrhythmogenic Right ventricular cardiomyopathy (ARVC) (formerly ARV Dysplasia – ARVD)
- Epsilon waves were absent in this case. If present, they are very specific, but are not sensitive.
- Usually with ARVD, there are right precordial T-wave inversion.
- ACM is characterised as a disease of the heart muscle, phenotyped by progressive fibrofatty replaceament that underlies the impairment of ventricular systolic function. This disease can implicate either the left or right ventricle (1).
- Scar-mediated ventricular tachycardia
- The arrhythmogenic substrate in ARVC is complex and heterogeneous. Structural abnormalities, including fibrofatty replacement, adipogenesis and scar border zones, create regions of non-uniform conduction that facilitate re-entry. Cellular heterogeneity, with varying proportions of diseased myocytes, fibroblasts, adipocytes and inflammatory cells further contribute to electrical instability. Desmosomal dysfunction promotes mechanical and electrical uncoupling, myocyte death and gap junction disruption, resulting in conduction slowing. Secondary abnormalities in sodium channel function, repolarisation and intracellular calcium handling , together with recurrent inflammatory episodes, further enhance arrhythmogenicity (2). Collectively, these structural and electrophysiological changes create a substrate prone to malignant macro-re-entrant ventricular tachycardia and ventricular fibrillation whilst driving progressive ventricular dysfunction (3).
The ECG suggests a highly arrythmogenic substrate:
- Primary repolarisation abnormalities, which suggest at least right ventricular involvement
- Right ventricular outflow tract-type PVCs, which may act as triggers for hetereogenous conduction through scar tissue and re-entry circuit VT to develop and sustain, degenerating into ventricular fibrillation
- Evidence of significant structural heart disease and possible biventricular involvement
Diagnosis:
- Biventricular Arrhythmogenic Cardiomyopathy
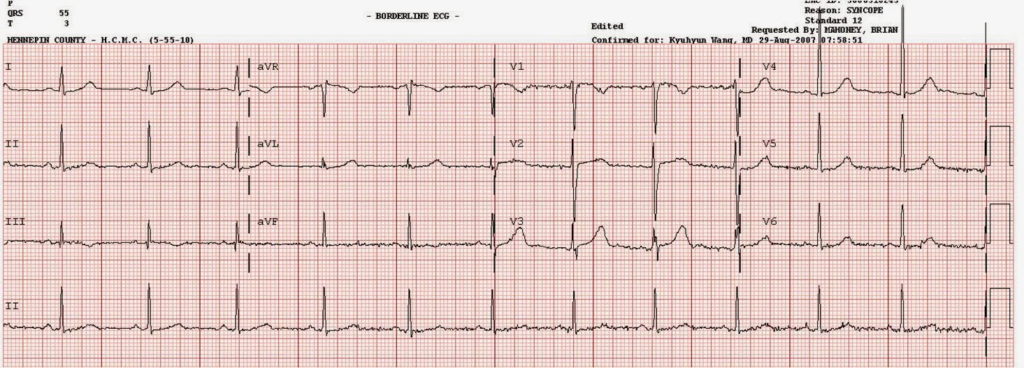
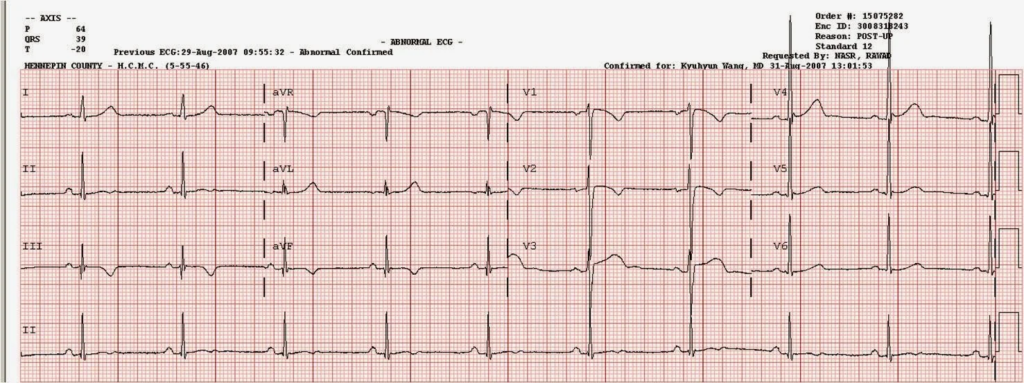
See 2 more cases and more information on RV cardiomyopathy (previously called arrhythmogenic RV dysplasia, or ARVD) (ECGs are pasted here for both cases).
Syncope in a young man (3 ECGs from the same patient)
= = =
Learning Points:
- VF Cardiac Arrest is most usually due to acute myocardial ischaemia, and one should have a low threshold to take to the cath lab, where OMI is suspected.
- Post-ROSC ECGs can mimic OMI. It is essential to get serial ECGs to watch for dynamic evolution.
- All forms of cardiomyopathy are substrates for causing cardiac arrest and must be considered in the initial workup from an arrest. The ECG forms a central part of this.
- Arrhythmogenic cardiomyopathy, formerly known as arrhythmogenic right ventricular cardiomyopathy, does and can involve both ventricles and one must assess the ECG holistically. The traditional epsilon wave may not form part of the surface ECG!
References
1. Corrado D, Zorzi A, Cipriani A, Bauce B, Bariani R, Beffagna G, et al. Evolving Diagnostic Criteria for Arrhythmogenic Cardiomyopathy. J Am Heart Assoc. 2021 Sep 21;10(18):e021987. doi:10.1161/JAHA.121.021987
2. Corrado D, Zorzi A, Cipriani A, Bauce B, Bariani R, Brunetti G, et al. Scarring/arrhythmogenic cardiomyopathy. Eur Heart J Suppl. 2023 May 1;25(Supplement_C):C144–54. doi:10.1093/eurheartjsupp/suad017
3. Andrews CM, Srinivasan NT, Rosmini S, Bulluck H, Orini M, Jenkins S, et al. Electrical and Structural Substrate of Arrhythmogenic Right Ventricular Cardiomyopathy Determined Using Noninvasive Electrocardiographic Imaging and Late Gadolinium Magnetic Resonance Imaging. Circ Arrhythm Electrophysiol. 2017 Jul;10(7):e005105. doi:10.1161/CIRCEP.116.005105
= = =
==================================
MY Comment, by KEN GRAUER, MD (7/9/2026):
Dr. Smith’s time-efficient approach to today’s case is so important — that I wanted to “walk through” his steps a 2nd time.
- The patient in today’s case is a young adult male who without trauma or prodrome — suddenly collapsed while playing football, and was found to be in VFib (Ventricular Fibrillation).
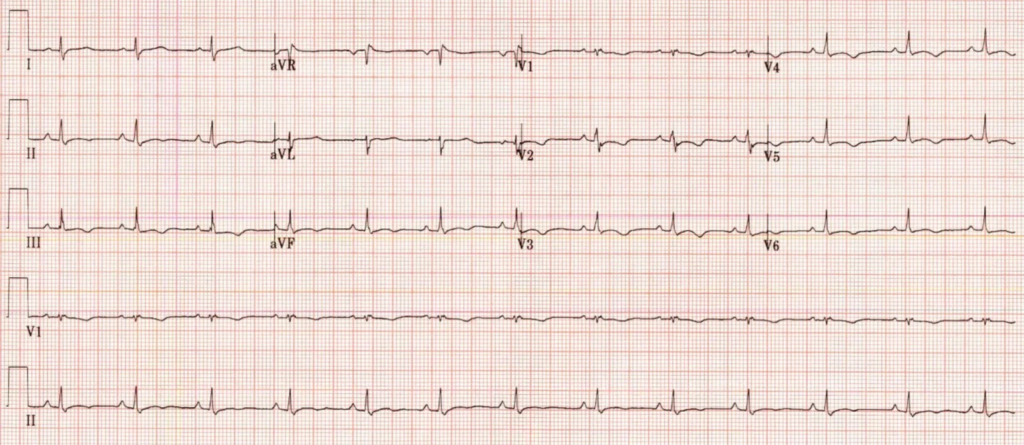
- ROSC was restored after 5 shocks. I’ve reproduced the initial post-resuscitation ECG that was recorded below in Figure-2.
KEY points in Dr. Smith’s assessment include the following:
- Although there are elements of potential ischemia in ECG #1 — the overall “picture” suggests severe pulmonary disease, and not acute OMI.
- Although prompt cardiac cath is not inappropriate in this scenario — awareness that the principal problem seems unlikely to be acute coronary occlusion is essential for optimal management, as this awareness shifts the focus toward assessing other reasons for this young patient’s unexpected cardiac arrest. I’ve listed the principal other reasons to consider below in Figure-1).
= = =
Figure-1: Causes of Sudden Death in Young Adults (References include Abbas et al: J Clin Med Res 15(1):1-9, 2023 — and — Tseng & Nakasuka: JAMA 333(11):981-996, 2025).
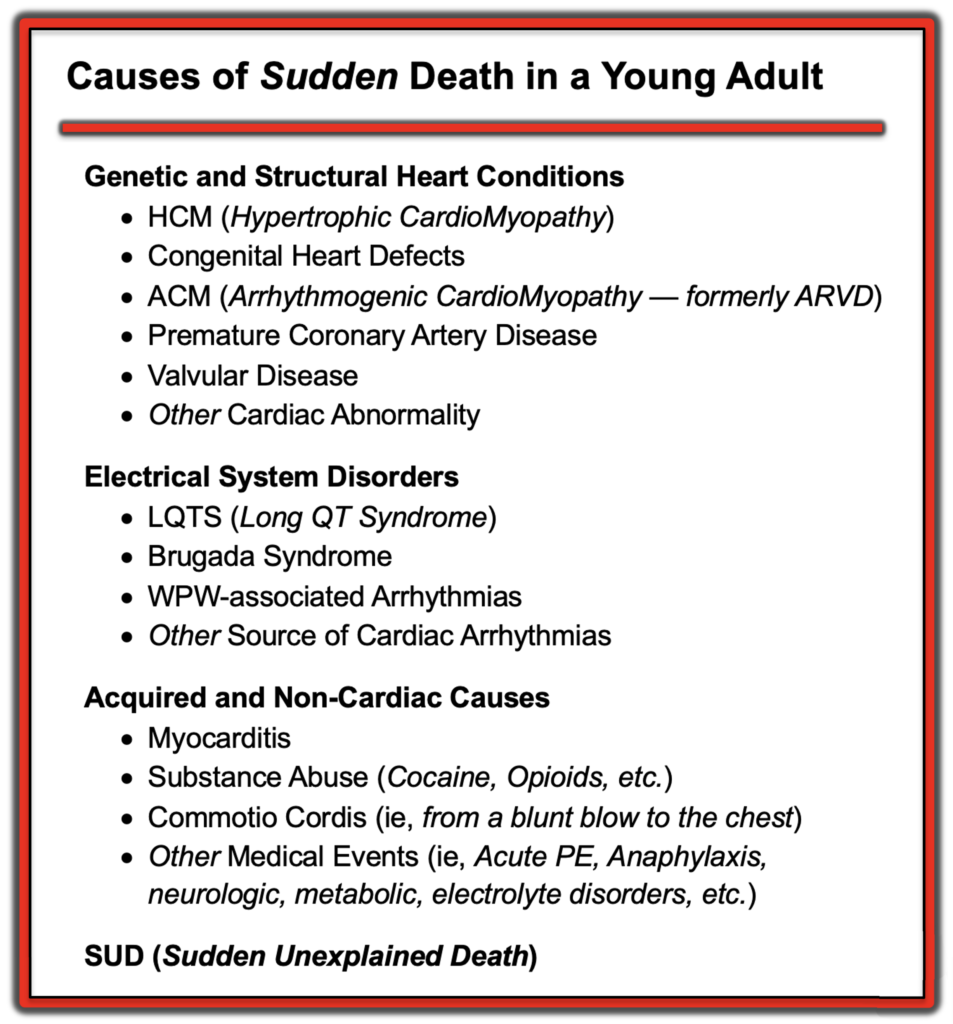
NOTE: As per Dr. Smith — the term “ARVD” (Arrhythmogenic Right Ventricular Dysplasia) has been replaced by ACM (Arrhythmogenic CardioMyopathy) in recognition of the fact that either the right and/or left ventricle may be involved to varying degree.
= = =
The Initial Post-Resuscitation ECG
Our “eye” tends to get used to what we are used to seeing — which is why it is sometimes difficult to recognize what we are not used to seeing. What we are not used to seeing in a patient with spontaneous onset cardiac arrest from VFib — is an ECG that looks like today’s initial ECG.
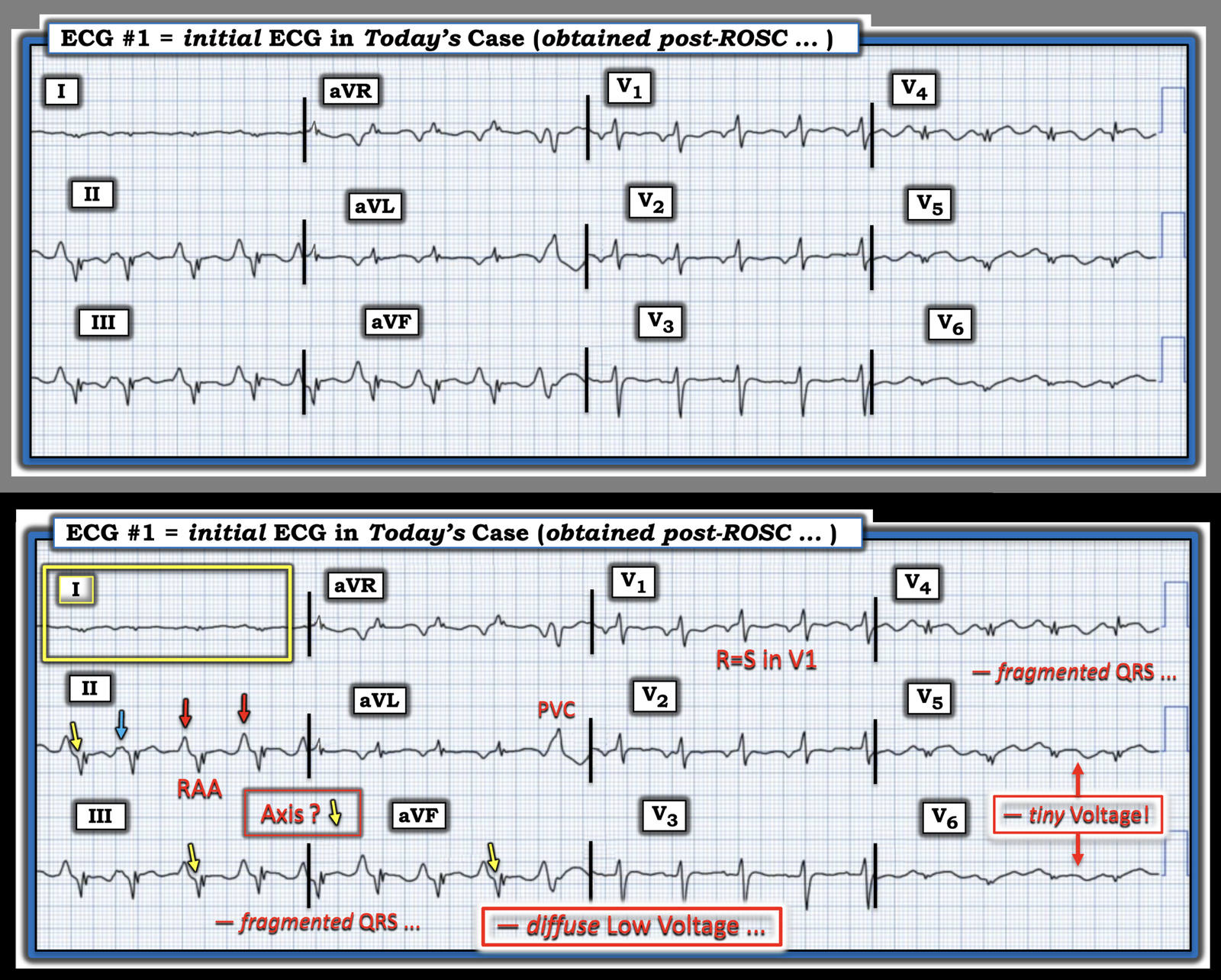
- To facilitate recognition — I’ve labeled in the lower panel of Figure-2 a series of KEY findings in the post-resuscitation ECG that should immediately convey a very different etiology than OMI for this patient’s arrest.
What strikes “my eye” in Figure-2:
- The rhythm is sinus tachycardia at ~110/minute (RED arrows in lead II highlight sinus P waves). The very tall and pointed nature of these sinus P waves tells us there is significant RAA (Right Atrial Abnormality) — and — this degree of RAA is almost uniformly associated with severe RVH (Right Ventricular Hypertrophy).
- Beyond-the-Core: There is a PAC (the BLUE arrow in lead II). In the context of marked RAA — I interpreted the notching in this BLUE arrow PAC as suggestive of biatrial abnormality (ie, both RAA and LAA).
- QRS amplitude is dramatically reduced! As noted in our review of the Causes of Low Voltage (CLICK HERE) — both myocardial “stunning”, as well as various types of cardiomyopathy figure prominently as potential etiologies! It is rare indeed to see as tiny voltage as we see in the lateral chest leads in Figure-2.
- As noted by Dr. Smith — Schamroth‘s Sign is prominently displayed by the negligible voltage of P wave, QRS and ST-T wave inlead I (within the YELLOW rectangle). Having looked for examples of Schamroth’s Sign over decades (ever since Barney Marriott brought my attention to this uncommon but insightful finding) — it is rare to see such true negligible voltage as is evident here in lead I (about the only other condition that might do this is bilateral arm-leg lead reversal, which is not present here). As in My Comment in the March 18, 2026 post — the presence of Schamroth’s Sign (especially in association with the marked RAA that we see in Figure-2) — instantly tells us there is some form of longstanding and severe pulmonary disease!
- Other ECG signs of severe pulmonary disease include: i) The indeterminate frontal plane Axis (predominantly negative QRS in each of the inferior leads with the null QRS in lead I); — ii) The R=S wave in lead V1 (normally the S wave predominates in V1); — iii) Global low voltage; — and, iv) S waves in multiple leads (See My Comment in the February 12, 2023 post — for “My Take” on RVH).
- In addition to all of the above — there is evidence of an ischemic contribution to this patient’s presentation, in the form of: i) QRS fragmentation (notching) in multiple leads (II,III,aVF; aVR,aVL; V4,V5,V6) — with this sign suggesting “scar” from longstanding disease; — ii) Deep and wide inferior lead Q waves (YELLOW arrows); — iii) The PVC; — and, iv) As per Dr. Smith — the hyperacute ST-T waves in the lateral chest leads. Taken together and considered in context — it is not surprising that this patient presented with shock and cardiac arrest .
= = =
BOTTOM Line:
ACM is not a common disorder in the general population. I went for years without seeing a case outside of what I read in textbooks. But as a source for receiving and sharing the cases we encounter — among younger adults who present with a malignant ventricular arrhythmia (as in today’s patient) — ACM (Arrhythmogenic CardioMyopathy) needs to be promptly considered on seeing an ECG like that shown in Figure-2 (See My Comment in the June 3, 2023 post — for more on ARVD/ACM).
= = =
Figure-2: I’ve labeled KEY findings in today’s initial ECG.
= = =
= = =