Submitted by Ali Khan MD, written by Pendell Meyers
A man in his early 50s presented with exertional chest pain and dyspnea. He had family history of early CAD. Otherwise, no clear risk factors. Vitals were within normal limits.
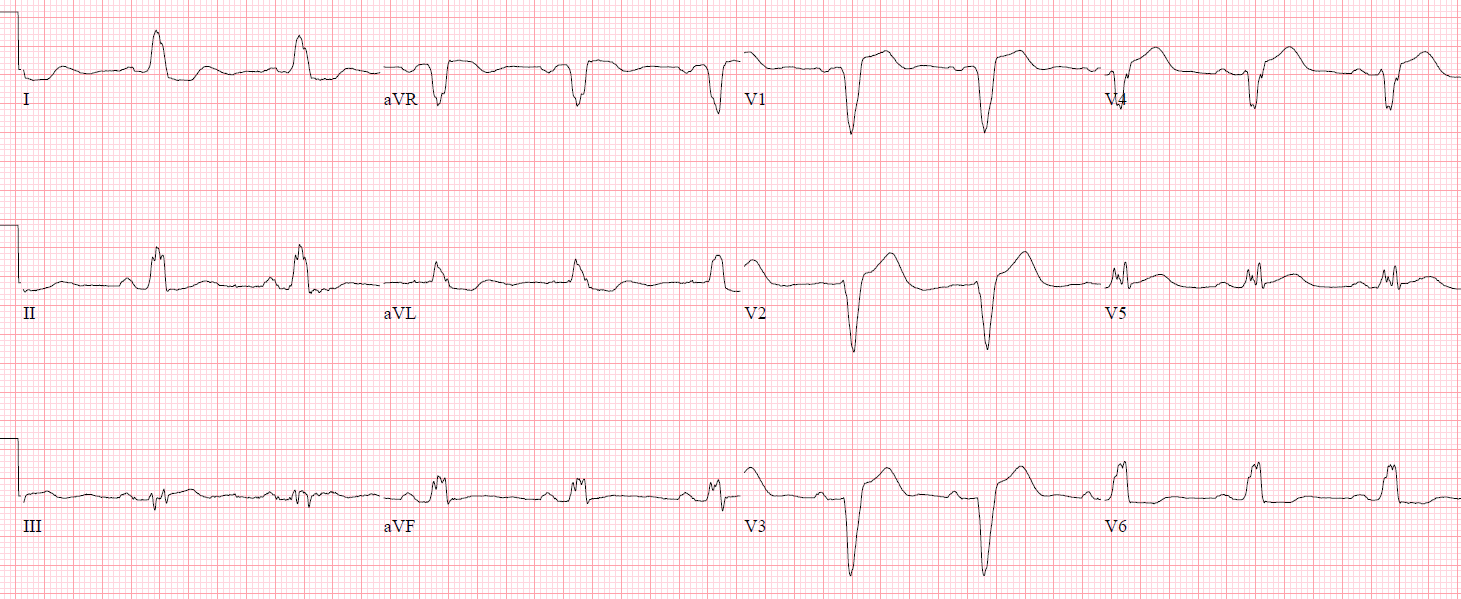
No prior ECG was available. Here is his triage ECG:
 |
| What do you think? |
This is yet another subtle inferior (and likely also posterior) OMI. There is a small and narrow QRS complex with reasonable axis and R wave progression, therefore the QRS cannot explain any abnormalities of the ST segment and/or T waves. The T waves in II, III, and aVF are subtly too large for their QRS, and the most important finding is that, in aVL, there is reciprocal STD and proportionally-large-volume T wave inversion (a “reciprocal negative hyperacute T wave”). There is also slight STD in I. The picture is not of perfect quality, but I believe there could be a hint of STD in V3-V4. Sinus brady at 60 bpm is another piece of evidence pointing to an RCA OMI, which supplies the SA and AV nodes, causing bradycardia and heart blocks during occlusion.
Dr. Khan immediately understood this ECG and called his cardiologist asking for emergent cath.
He also sent this picture to me in real time with no information at all, and I responded: “It is diagnostic of inferior OMI to me. But it will be a hard sell to most cardiologists.” This was not meant to be critical of cardiology, but it does reflect my truthful expectation based on prior experience and cases that we are sent from all over the world. Most people, EM or cardiology or other specialty, cannot see this subtle STEMI(-) OMI.
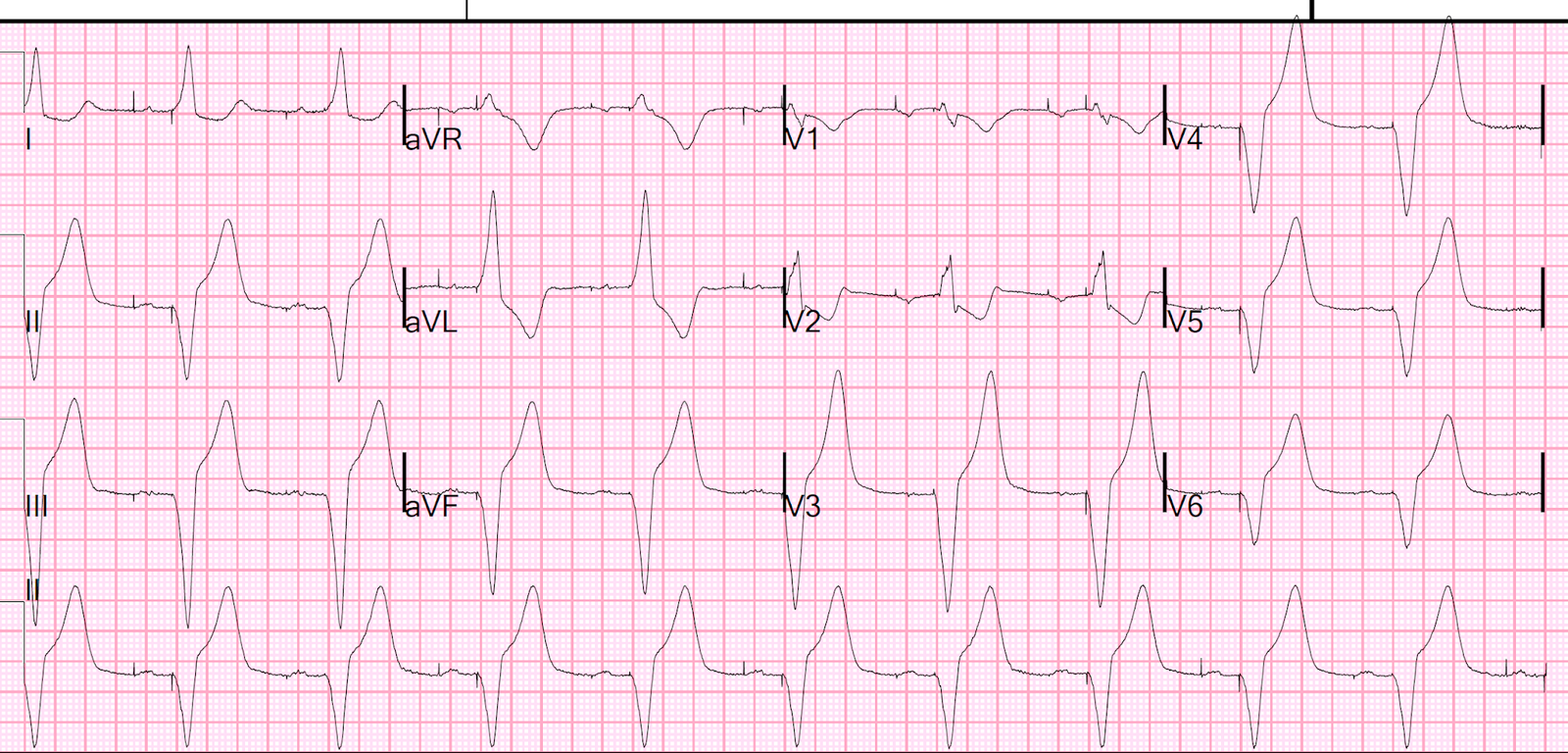
Here is a zoomed-in picture of the inferior leads showing that it truly does not meet STEMI criteria (although humans have never been able to agree on measuring STE anyway):

Dr. Khan and the interventionalist on call agreed that this patient needed emergent cath.
A complete acute occlusion (TIMI 0) of the RPL (right posterolateral artery), requiring 3 stents to restore TIMI 3 flow.
The high sensitivity troponin I returned at 1468 ng/L. No further troponins were measured.
Echocardiogram showed an inferior wall motion abnormality.
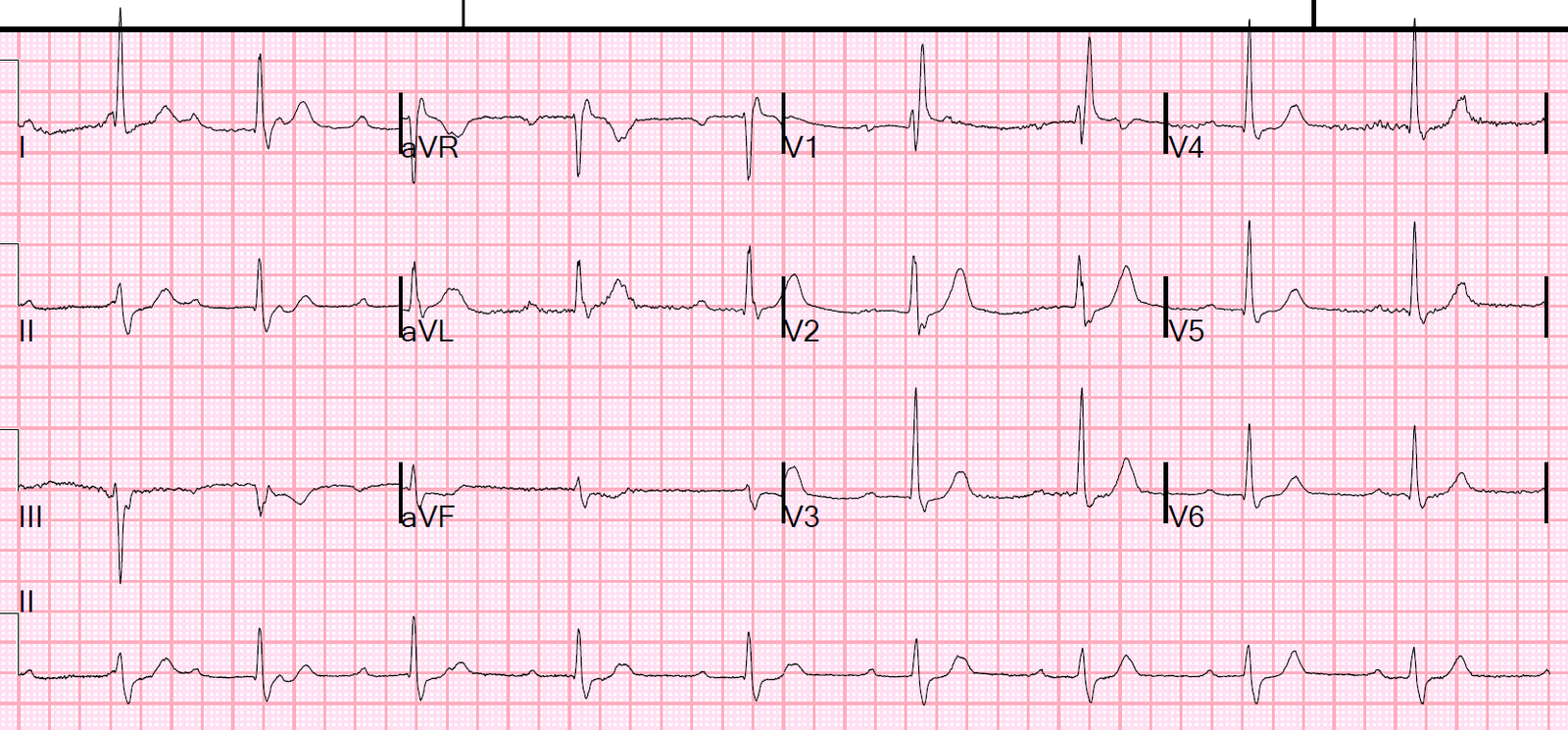
Here is his ECG after the intervention:
 |
| There are up-down biphasic T-waves in III and aVF. There are enlarged upright T-waves in V2 and V3 These are all findings which reflect reperfusion of the inferior and posterior walls. |
The patient did well.
Learning Points:
Hyperacute T waves are not well defined, but involve an increased size/bulk/area of the T wave compared to the QRS complex, and compared to prior T waves if available. They of course cause reciprocal findings on the opposite wall.
aVL is a reliable reciprocal partner for lead III. When there is OMI in one of these two areas, the other lead will reliably show reciprocal findings. In this case, I need lead aVL (showing reciprocal negative hyperacute T waves) to be sure that the inferior T waves are hyperacute.
Check out these other cases of subtle inferior OMI where aVL is very helpful:
This patient with “NSTEMI” was not allowed to go to the cath lab. Then the ED provider obtained an emergent coronary CT angio. What do you think it showed?
A woman in her 60s with chest pain and prominent J waves
A man in his 50s with 2 hours of chest pressure
60-something with 2 days of intermittent epigastric pain. Why does the cardiologist disagree?
A 40 yo with Chest pain. Only ECG abnormality is minimal ST depression in I and aVL (computer interpretation: normal)
You have two hours to save this patient’s life
This ECG was shown to the doctor with no clinical information
A male in his 60s with chest pain
See this great post for some examples of high lateral OMI and compared to some false positives: