===================================
MY Comment by KEN GRAUER, MD (7/28/2020):
===================================
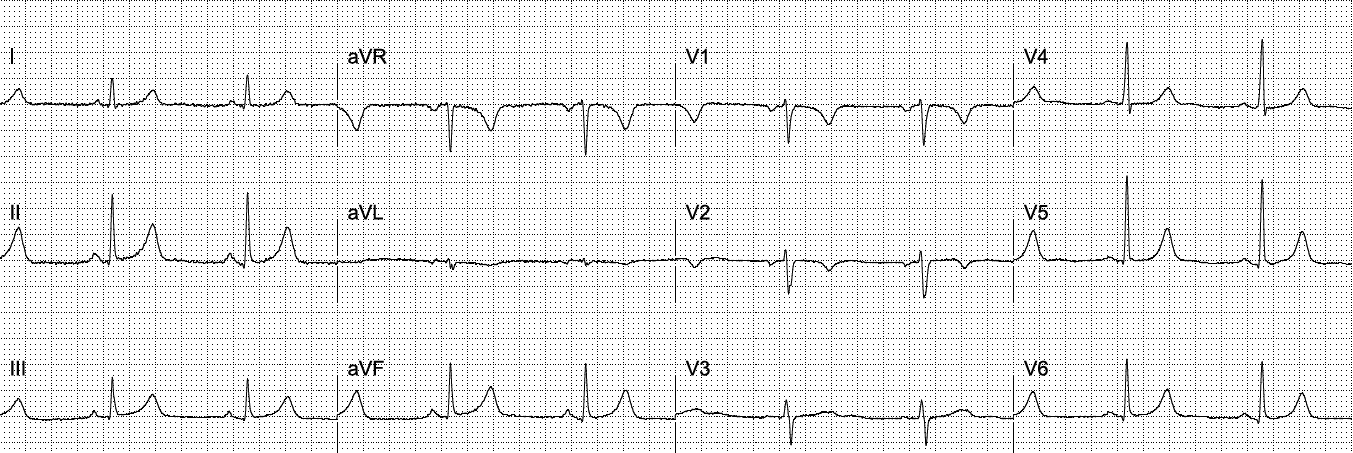
The ECG in Figure-1 was obtained from a middle-aged woman who presented to the ED with new-onset shortness of breath.
- QUESTION: Is the inferior lead T wave inversion indicative of RV (Right Ventricular) Strain from acute PE (Pulmonary Embolism)?
 |
| Figure-1: ECG obtained from a middle-aged woman who presented to the ED with new dyspnea (See text). |
MY THOUGHTS on ECG #1: As always — I favor a systematic approach to ECG interpretation. Without a systematic approach — it might be all-too-easy to overlook that something is “off” here …
- Regardless of whichever systematic approach you favor for 12-lead ECG interpretation — the 1st Step should always be to interpret the rhythm. Once you’ve ensured that your patient is hemodynamically stable — the, “Watch Your Ps, Qs and 3Rs” memory aid reminds me of the 5 KEY parameters to assess (CLICK HERE — if interested in more on this Ps, Qs, 3R approach).
- Although there is no long lead rhythm strip in ECG #1 — the rhythm is regular at a rate of ~80/minute. The QRS complex is narrow.
- P waves are present — and, these P waves are clearly related to neighboring QRS complexes, because the PR interval is constant. This tells us that P waves are conducting to produce the QRS complex that follows them.
- Did you recognize that the P wave in lead II is negative?
PEARL #1: If you see P waves that are conducting, but these P waves are negative in lead II — then you do not have a sinus rhythm. The only 2 exceptions to this are: i) If there is dextrocardia; and/or, ii) If there is some type of lead reversal.
- PEARL #2: We can easily rule out dextrocardia for ECG #1 — because R wave progression is perfectly normal in the chest leads (there should be reverse R wave progression if the patient had dextrocardia).
- This leaves us with distinguishing between a low atrial or junctional rhythm (which could be the cause of negative P waves in lead II) — vs some type of lead reversal.
Recognition of Lead Reversal:
Technical errors featuring a variety of lead reversal placements remain a surprisingly common “mishap” of everyday practice. As a result — we like to periodically publish clinical examples of lead misplacement. To review a number of these — GO TO:
- The March 18, 2020 post.
- The February 11, 2020 post.
- The November 4, 2018 post.
- The July 29, 2018 post.
- — and, this future post from August 28, 2020 (LA-LL Reversal).
PEARL #3 — I’ve summarized in Figure-2 those tips that have helped me most over the years to rapidly recognize tracings in which lead reversal is likely (Taken from My Comment in the February 11, 2020 post in Dr. Smith’s ECG Blog).
- Applying the tips from Figure-2 to the initial ECG in Figure-1 — not only is the P wave negative in lead II — but lead aVR does not manifest a predominantly negative QRS complex. Instead, the QRS in lead aVR appears to be positive and both the tiny P wave and T wave in this lead also appear to be positive. This shouldn’t normally be …
- Increasing my suspicion further that there must be some type of lead reversal in ECG #1 — is the overly similar appearance of the QRST complex in all 3 of the inferior leads.
- By far — the most common lead reversal is mix-up of the LA (Left Arm) and RA (Right Arm) electrodes. But this is not the mix-up that occurred in today’s case — because we do not see global negativity (of P wave, QRS and T wave) in lead I (See the February 11, 2020 post).
 |
| Figure-2: Tips for recognizing lead reversal. (See text). |
PEARL #4 — My favorite on-line “Quick GO-TO” reference for the most common types of lead misplacement comes from LITFL ( = Life-In-The-Fast-Lane). I have used the superb web page they post in their web site on this subject for years. It’s EASY to find — Simply put in, “LITFL Lead Reversal” in the Search bar — and the link comes up instantly.
- This LITFL web page describes the 7 most common lead reversals. There are other possibilities (ie, in which there may be misplacement of multiple leads) — but these are less common and more difficult to predict.
- When I suspect a type of lead reversal that I am less familiar with — I simply review those 7 most common types of lead reversal on the LITFL page — and see if any of the ECG examples they provide seems to apply. In ECG #1 — the key identifying feature that led me to suspect RA-LL reversal was the finding of similar-looking global negativity in each of the 3 inferior leads (See Figure-3).
 |
| Figure-3: Features of RA-LL Lead Reversal — adapted from LITFL (See text). |
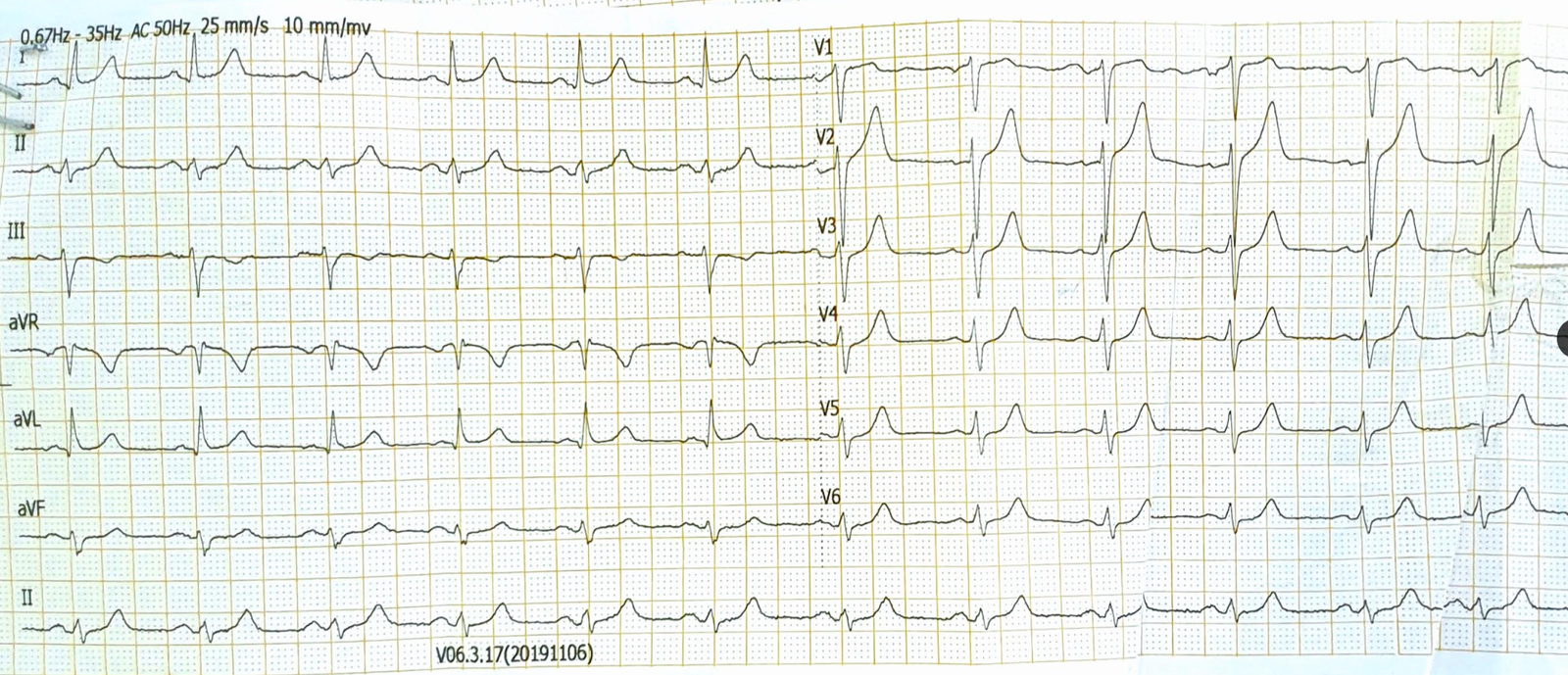
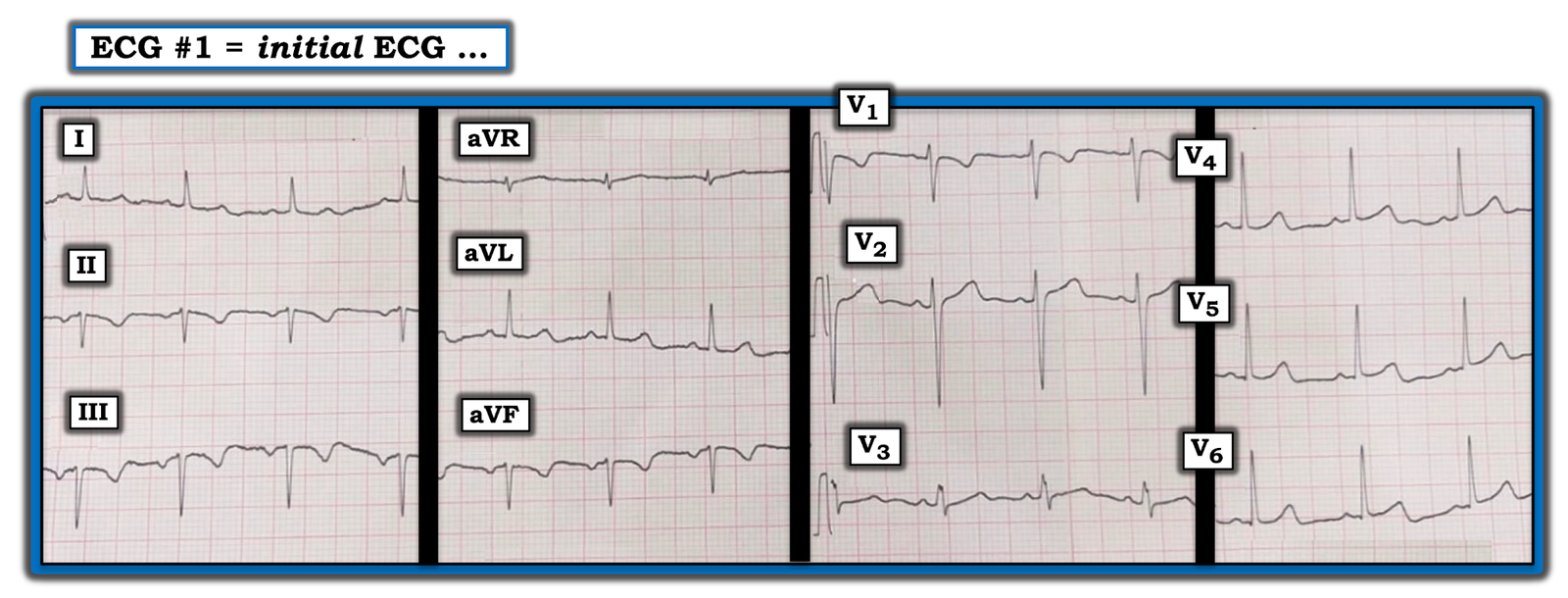
With the essentials from Figure-3 of RA-LL lead reversal in mind — Let’s TAKE ANOTHER LOOK at the initial ECG in this case (TOP tracing in Figure-4):
 |
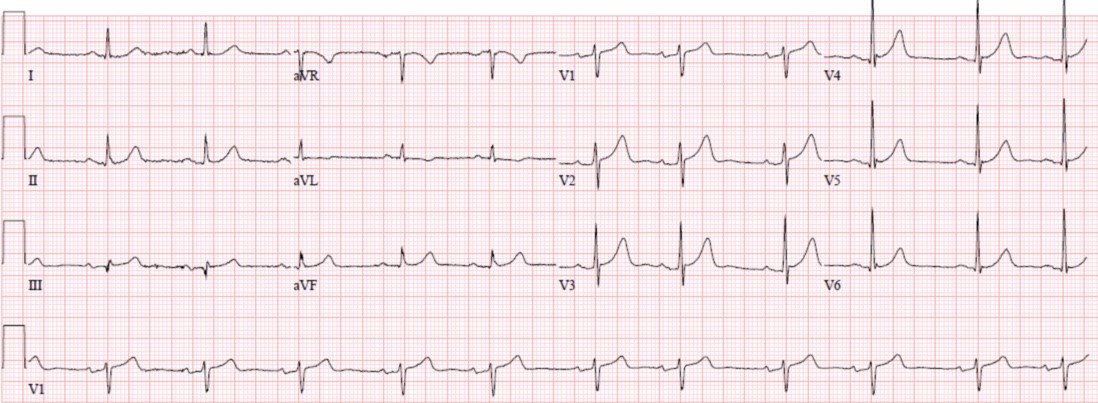
| Figure-4: TOP: The initial ECG in the ED ( = ECG #1) — with features of RA-LL lead reversal written below ECG #1. BOTTOM: ECG #2 shows what this initial ECG would look like if corrections were made for RA-LL Lead Reversal (See text). |
MY THOUGHTS on ECG #2: Unfortunately (as often occurs) — RA-LL lead reversal went unrecognized in today’s case. As a result, I do not have an actual follow-up ECG. Instead — I constructed ECG #2 in Figure-4 by inverting lead II in ECG #1 — by inverting and switching places for leads I and III — and by switching places for leads aVR and aVF. Isn’t the appearance of P waves, QRS complexes and T waves in the limb leads of ECG #2 now much more logical?
- The P wave is upright in lead II of ECG #2, as it should be when there is normal sinus rhythm.
- There is global negativity (of P wave, QRS and T wave) in lead aVR — as most commonly is seen with normal tracings.
- The appearance of the P waves, QRS complexes and T waves no longer looks so similar in the 3 inferior leads in ECG #2, as it did in ECG #1 when there was RA-LL lead reversal.
- My Impression of ECG #2: This is a normal ECG. There is normal sinus rhythm — a horizontal (but normal) frontal plane axis of about 0 degrees — and no chamber enlargement. T wave negativity isolated to lead III is not an abnormal finding when the QRS complex is predominantly negative in this lead. There is no longer suggestion of RV strain, since the T wave in leads II and aVF is upright. As stated earlier — R wave progression in the chest leads is normal. T wave inversion isolated in the chest leads to lead V1 is not abnormal. In Summary — This is a normal ECG.
![]()