Case submitted and written by James Tavornwattana, edits by Pendell Meyers and Steve Smith.
A male in his 60s with diabetes presented to the ED with one hour of palpitations associated with a 30 min episode of throat burning
sensation when he woke up this morning. He denied chest pain, shortness of breath, or lightheadedness.
= = =
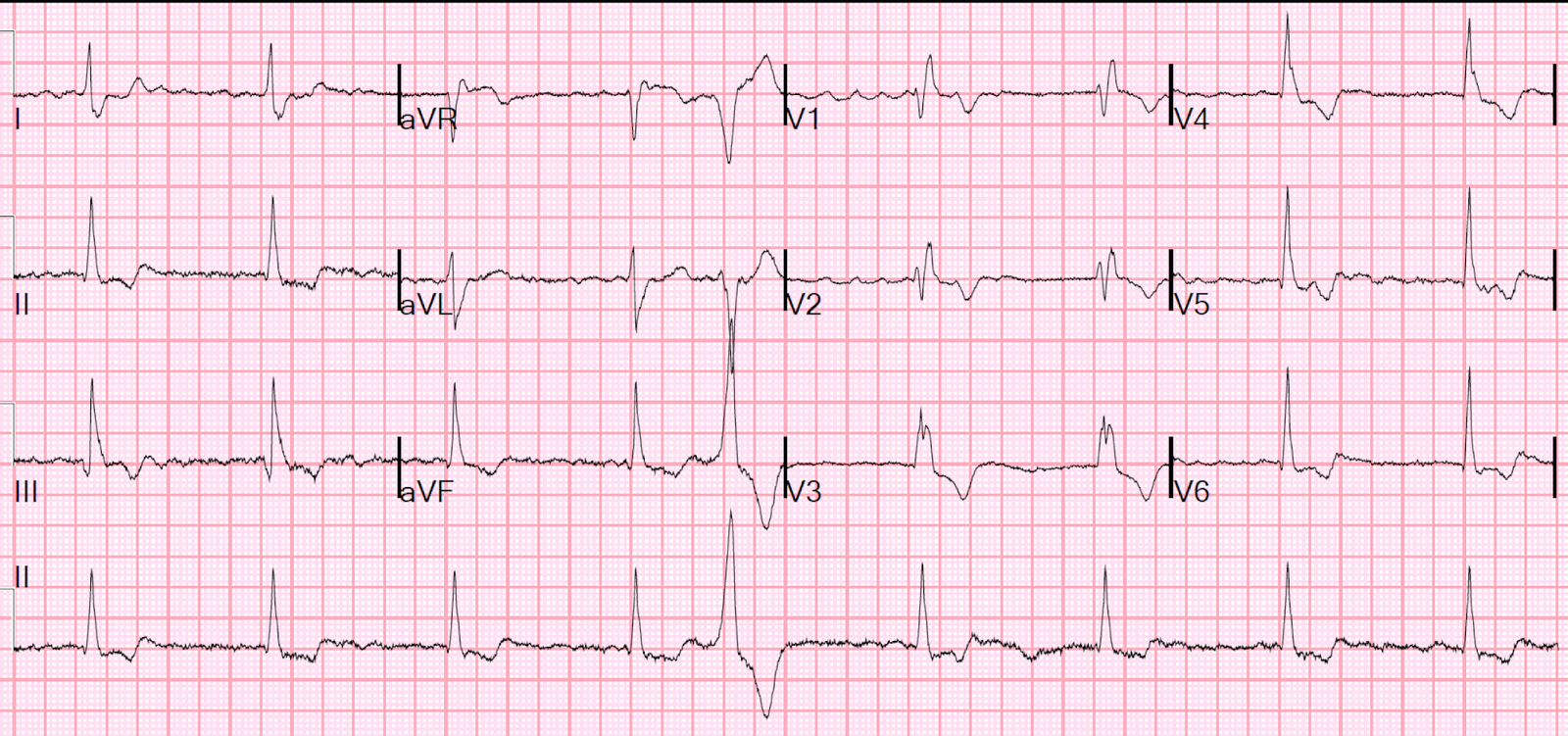
Initial ECG (0 hr):

What do you think?
= = =
Interpretation:
- Atrial fibrillation with rapid ventricular response.
- ST depression that is maximal in V2-V4, also with lesser STD in V5, I, aVL, II and aVF. With multi-lead STD, there is of course STE in aVR.
In sinus rhythm, this pattern and location of STD (maximal in V1-V4) is indicative of focal, posterior transmural infarction, with the most likely etiology being Occlusion MI. Notably, this is NOT the pattern of diffuse supply/demand mismatch, in which the STD is maximal in V4-6 and lead II.
- There are other possibilities, such as a “type II STEMI”, for example: acutely increased demand (in this case due to rapid ventricular response) on an already chronically stenosed LCX, resulting in massive supply/demand mismatch and transmural ischemia. But this would be a diagnosis of exclusion compared to the possibility of OMI, given the diagnostic ECG.
Smith: In the presence of atrial fibrillation with RVR, it is much less definitive. STD max V1-V4 can be due to subendocardial ischemia. Management is to electrically cardiovert (this is an emergency!) and then re-evaluate when in sinus rhythm.
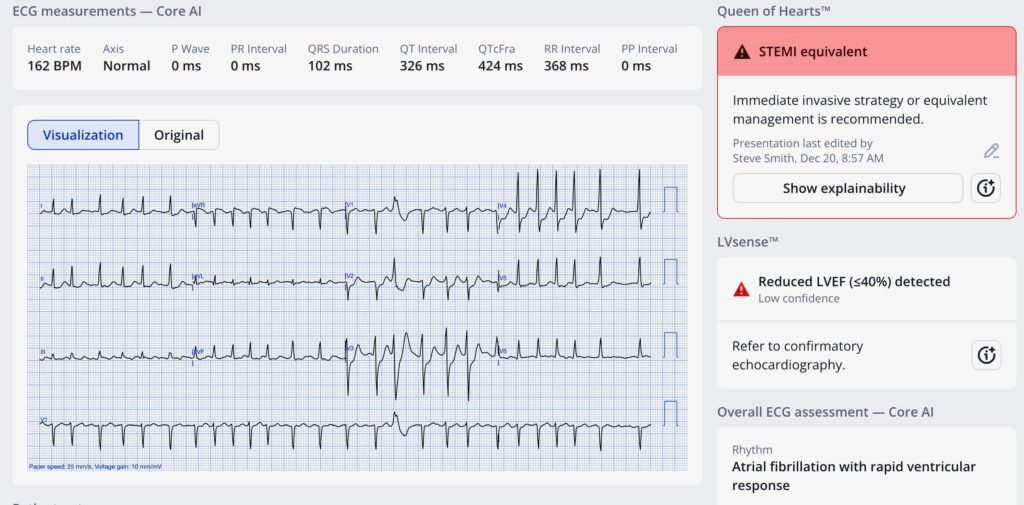
Smith continues: In this case, the STD is very deep, and so subendocardial ischemia is less likely than OMI. Indeed, when submitted to the Queen of Hearts, she diagnosed OMI. For contrast, see this case from Nov 23 2025, in which STD V1-V4 was much less profound, and all due to atrial fibrillation with RVR, and the Queen of Hearts got it right (Not OMI).
What does the Queen say for this one?? Here she is:
= = =
Back to the case:
The clinicians thought the STD represented demand ischemia from AF with RVR. The patient was given magnesium, diltiazem, and fluids with improvement in ventricular rate. Unfortunately there is no ECG recorded soon after rate control. This would be important to see if the posterior ischemia has resolved with rate control or not.
- The 1st troponin T was negative (less than 0.01 ng/mL) and the patient was admitted to the cardiology unit.
The 2nd troponin T returned at 0.20 ng/mL, and a repeat ECG was ordered at around 8 hours after presentation:

= = =
Interpretation of the Repeat ECG:
- The patient has converted back to sinus rhythm. Still slight STD in V3-V5, but otherwise the findings of OMI are much improved compared to the initial ECG. We do not know if the patient still had active pain at this time, but I would suspect that this ECG represents reperfusion (or collateral circulation).
Smith: This suggests that there was type 2 ischemia, not ACS. But it is not definitive. Such profound Type 2 ischemia would require significant coronary stenosis, so an angiogram is indicated, but emergent angiogram is not necessary.
- Troponins continued to rise, with peak 0.67 ng/mL at about 24 hours from presentation.
- Echo showed moderate-to-severe mid-to-basal inferolateral wall hypokinesis (what is commonly referred to as the posterior wall).
= = =
Apparently at this time, the patient was no longer symptomatic. As a result — cath was scheduled for the next morning.
- The cath showed a complete thrombotic occlusion of the LCX (collateral flow was not commented on, but could have been present).
- The LCX was stented open with good angiographic result.
- There was also other chronic CAD in various vessels without any other acute culprits.
Here is the post-cath ECG:

= = =
Interpretation of the post-cath ECG:
- Roughly the same as before the cath.
= = =
The patient did well.
= = =
Learning Points:
- When there are multiple leads with STD, then you must find where the STD is maximal. STD maximal in V1-V4 is posterior OMI until proven otherwise.
- Diffuse supply/demand mismatch ischemia presents with STD maximal in V4-V6 and lead II (the average overall axis of depolarization), and therefore must always also present with STE in aVR.
Smith: The exception is atrial fib with RVR, which may present with STD max in V1-V4. Cardioversion is indicated for such a case.
- See this diagram that highlights this learning point:

= = =
When ECG findings of OMI are present in the setting of AF with RVR, one of the initial steps in management is to control the rate which will reduce supply demand mismatch and allow for a repeat ECG at reduced heart rate (with better quality and the chance to see if the ischemic findings have resolved with reduced rate).
See this similar case:
A middle aged man with ST depression and a narrow window of opportunity
= = =
= = =