A woman was found outside with altered mental status.
She was GCS 3. BP 80/40
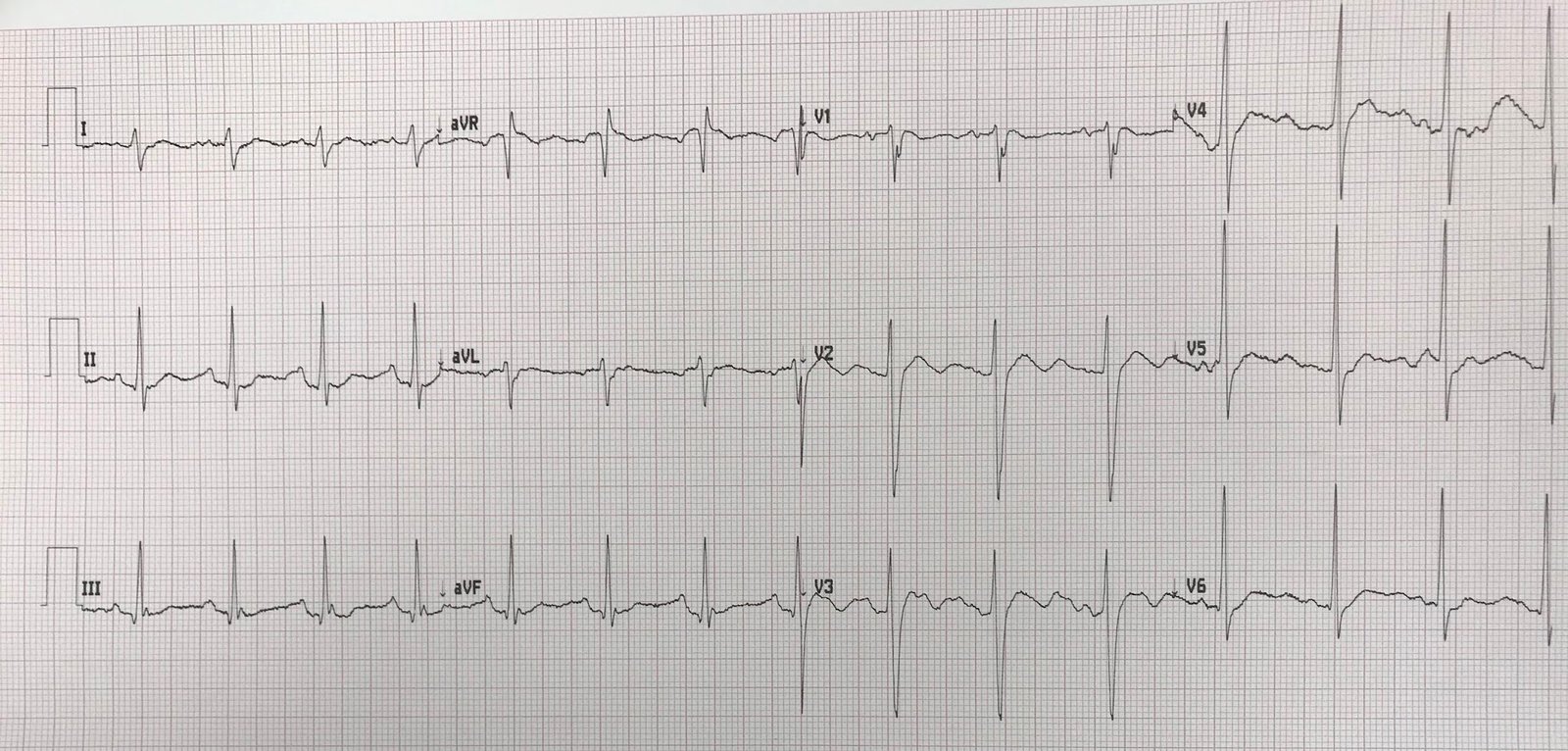
Here is her ECG:
 |
| Diagnosis? |
Sinus bradycardia with Osborn waves. Temperature was 24.3 degrees Celsius.
She was intubated (carefully, so as not to irritate her heart into ventricular fibrillation).
She requires internal rewarming at this temperature. External rewarming would be dangerous, as it results in both rewarming shock (hypotension/shock due to shunting of core blood flow to the surface) and “core afterdrop”(shunting of cold surface blood to the core, dropping core temperature).
Because she has an appropriate blood pressure and perfusion, bypass or ECMO is not necessary at this point (but still might become necessary).
This patient was rewarmed with thoracic cavity lavage and intravascular catheter, the same used for induced therapeutic hypothermia. In this case, the Alsius catheter was placed. The patient was warmed and did well.
![]()
===================================
MY Comment by KEN GRAUER, MD (1/2/2020):
===================================
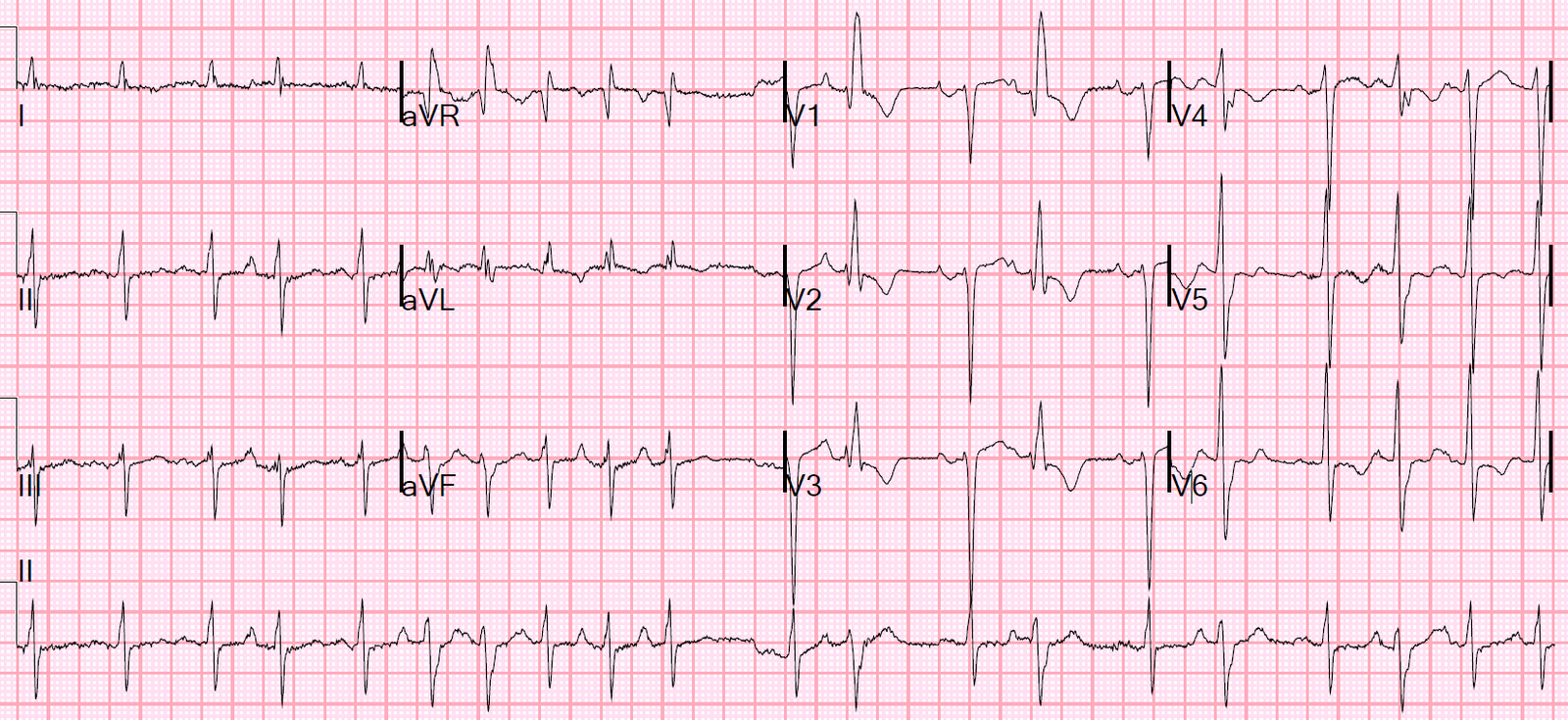
This case provides an excellent example in which the History + recognition of Osborn Waves provide the essential clues to facilitate an instant diagnosis of severe Hypothermia. That said, in addition to bradycardia + Osborn waves — there are 2 other ECG findings in Figure-1 that should be noted and followed up after correction of hypothermia.
QUESTION: What are these 2 additional ECG findings?
- HINT: Were you systematic in your interpretation? Or, did you “jump” at the diagnosis of hypothermia without first surveying the entire tracing?
 |
| Figure-1: The ECG shown in this case (See text). |
Systematic Interpretation of ECG #1:
- Rate & Rhythm — There is marked sinus bradycardia at ~48/minute.
- Intervals — The PR interval is not prolonged (ie, not more than 0.20 second). The QRS complex is narrow (ie, not more than half a large box = 0.10 second in duration). However, the QTc interval is clearly prolonged! This is the 1st additional ECG finding that should be noted. I measure a QT interval of ~590 msec (my measurement in lead V3). Because of the very slow heart rate — the actual QTc will be less than this amount — but the QTc will still be markedly prolonged!
- Axis — Normal (about +50 degrees).
- Chamber Enlargement — None.
- Q-R-S-T Changes — There are small and narrow q waves in multiple leads. Transition occurs early (ie, the R wave becomes taller than the S wave is deep between lead V1-to-V2). There is at least 1-2 mm of ST elevation in multiple leads (ie, leads II, III, aVF; V2-thru-V6). This is the 2nd additional ECG finding that should be noted.
- Finally — There are prominent Osborn Waves in multiple leads (RED arrows in ECG #1).
OSBORN Waves: The Osborn wave has been described as a deflection with a dome or hump that occurs at the point where the end of the QRS complex joins with the beginning of the ST segment. This is the J-Point (ie, it Joins the end of the QRS with the beginning of the ST segment) — so Osborn waves are exaggerated J-point waves. They’ve also been called the “camel-hump” sign.
- Osborn waves are most commonly associated with significant hypothermia (usually not seen until core temperature is below 90°F). Given the History in this case (ie, in the middle of winter, this patient was “found outside” in shock, and with altered mental status) — as soon as you “touch” this undoubtedly “cold” patient, you’ll KNOW the diagnosis.
- PEARL — It is important to appreciate that other conditions may also be associated with prominent J-point deflections. Osborn waves have been reported with hypercalcemia, brain injury, subarachnoid hemorrhage, Brugada syndrome, cardiac arrest from VFib — and — severe, acute ischemia resulting in acute MI. The development of Osborn waves in association with acute ischemia/infarction may be a marker of impending VFib (See the 11/22/2019 post on Dr. Smith’s blog).
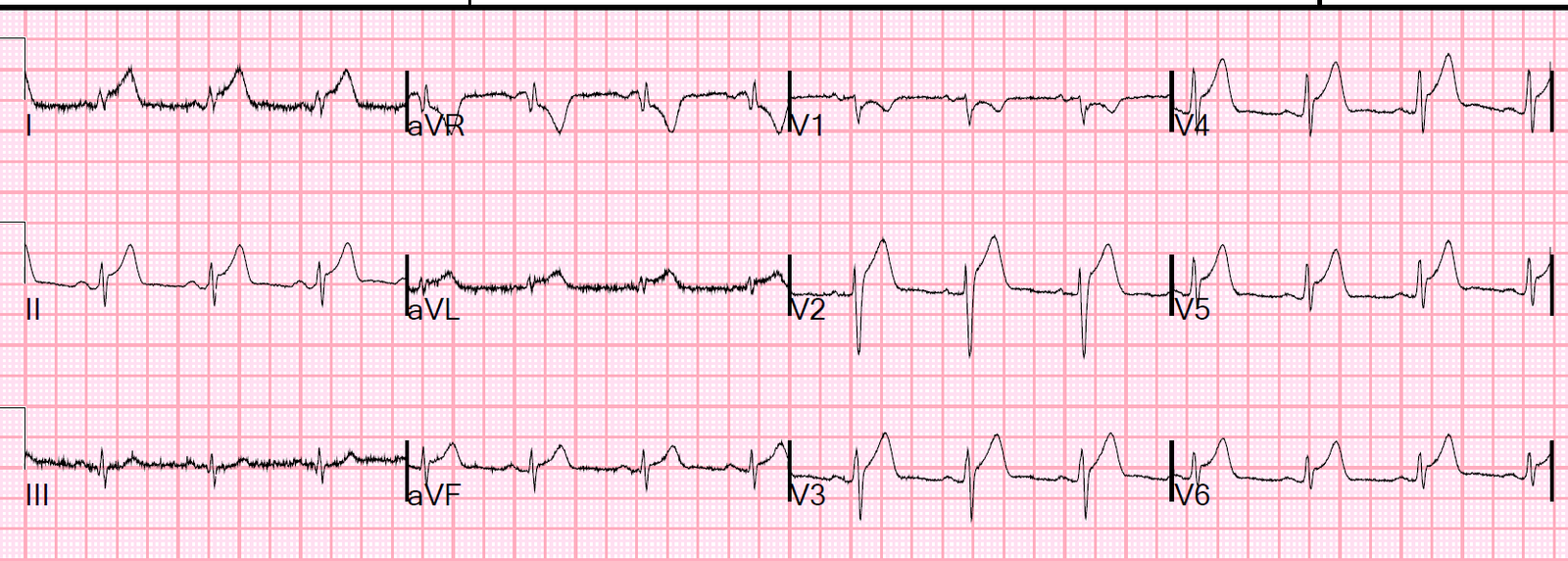
FINAL THOUGHT: As emphasized by Dr. Smith — highest priority in this case is internal rewarming. After that has been accomplished — the ECG should be repeated!
- It is highly likely that all 4 of the important findings in this case resulted from this patient’s profound hypothermia. I would expect normalization of the heart rate and QTc interval — along with resolution of Osborn waves and the diffuse ST elevation. BUT — one never knows — and prudence dictates ensuring that the QTc does normalize, and that ST elevation is less (and does not look worrisome) after return to a more normal core temperature.
- CLICK HERE — for a similar case in which bradycardia, QTc prolongation, Osborn waves, and diffuse ST elevation all resolved after correction of hypothermia.
Out THANKS to Dr. Smith for presenting this case!
![]()