This is a very commonly missed ECG of a terrible condition. In this case, it was almost dismissed. I present many other similar ECGs at the bottom that were indeed missed or dismissed.
Case
I was texted this ECG from a physician assistant who works by himself in several small Emergency Departments.
He is a particularly smart and well trained emergency medicine PA (because he trained at Hennepin).
He added the words:
“What do you think? 70-something male with DM, HTN, no previous MI, with Chest pain”
 |
| What do you think? |
Here was my response:
“Definite Huge Occlusion MI (OMI). STEMI! This is a bad one. There is RBBB with Left Anterior Fascicular Block (LAFB) which is a very ominous sign.”
He texted back:
“That’s what I thought but the cardiologist (at the receiving facility) was not convinced.”
This is an obvious diagnosis to me. Unambiguous. Can’t be anything else.
There is RBBB with LAFB with huge ST Elevation seen in V2-V4, (also subtle STE in aVL).
(The rhythm is uncertain, but it is supraventricular and probably atrial bigeminy (with P-waves that are not well seen), but the rhythm diagnosis is NOT critical in making the OMI diagnosis.)
Here I have put a line at the end of the QRS and beginning of the ST segment, so that you can assess for ST Elevation:
 |
| The image is distorted because it was a photo of a paper ECG.
That is why the lines are not parallel. Also note that the Elevated ST Segments in V2 and V3 are downsloping. In the many cases of RBBB + LAFB in anterior MI that I have seen, this is the rule rather than the exception. |
Case continued:
The PA transferred the patient and, on arrival, the ECG was reportedly even more obvious. The patient went to the cath lab:
Proximal LAD: 90% with thrombus
Mid LAD: 80% with thrombus
Distal LAD: 80% with thrombus
3 stents were placed. Peak hs Troponin T was 23,070 ng/L (equivalent to 23 ng/mL; this is an enormous infarct!).
Echo showed anterolateral and septal wall motion abnormalities and an ejection fraction of 29%.
Comment:
Some ECG findings which are very clear to me are not clear to others. I try not to post cases that are easy. This one I would have thought was easy. But apparently it is not, as ECGs like this are very often missed, by all kinds of providers, including cardiologists.
More similar cases
Other examples of RBBB/LAFB OMI in which the cardiologist contradicted the interpretation of the emergency provider and disagreed with cath lab activation:
I had just resuscitated this patient from VF cardiac arrest after 68 minutes of CPR:
 |
I told the cardiologist that it is a proximal LAD occlusion and he rolled his eyes, and said “Maybe.” It was indeed acute LAD OMI |
____________________________
Here is another example in which the cath lab was activated, then de-activated by the cardiologists, with the ST Elevation annotated below it:
This patient died 8 hours after cath lab de-activation.

With markup
 |
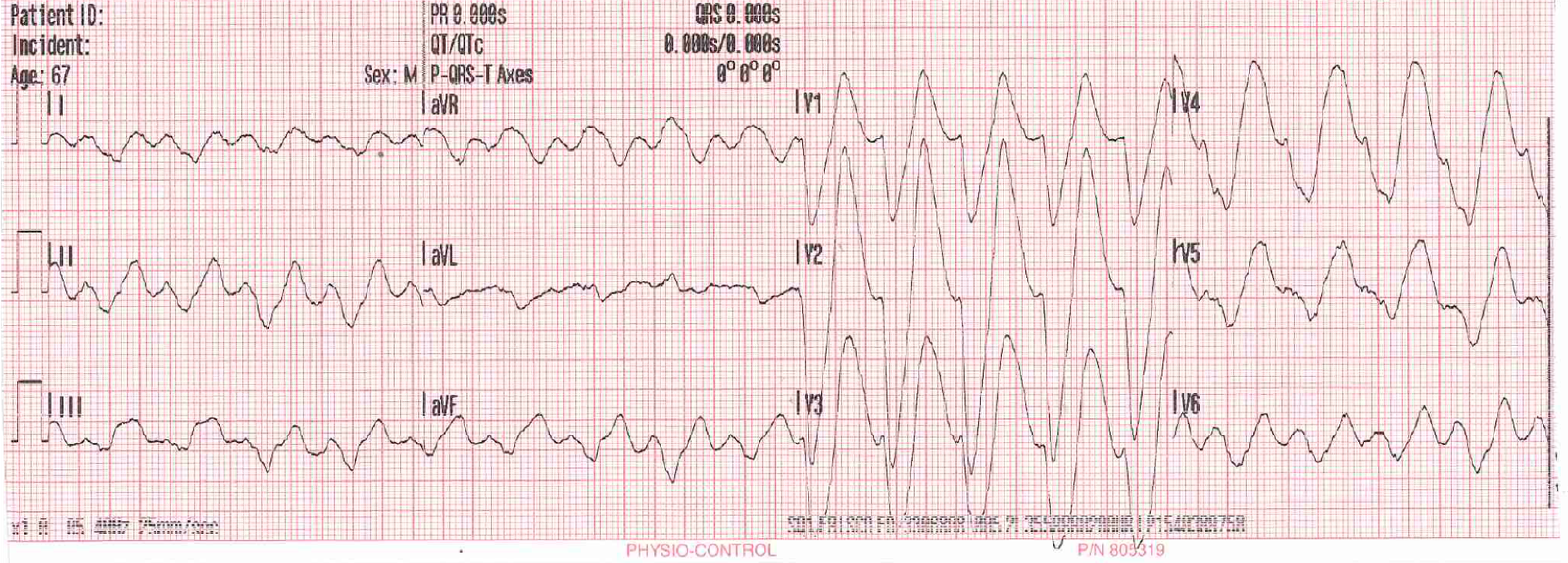
Wide Complex Tachycardia; It’s really sinus, RBBB + LAFB, and massive ST elevation |
_________________________
Here is another that was missed:
 |
Resuscitated from ventricular fibrillation: what is the ECG Diagnosis? |
________________________
Finally, this one
Here is a case of a young woman who presented with acute pulmonary edema. The ECG was recorded during the pulmonary edema. Cath lab was activated, then she arrested, and, after 30 minutes of resuscitation, achieved ROSC but was in severe shock.
 |
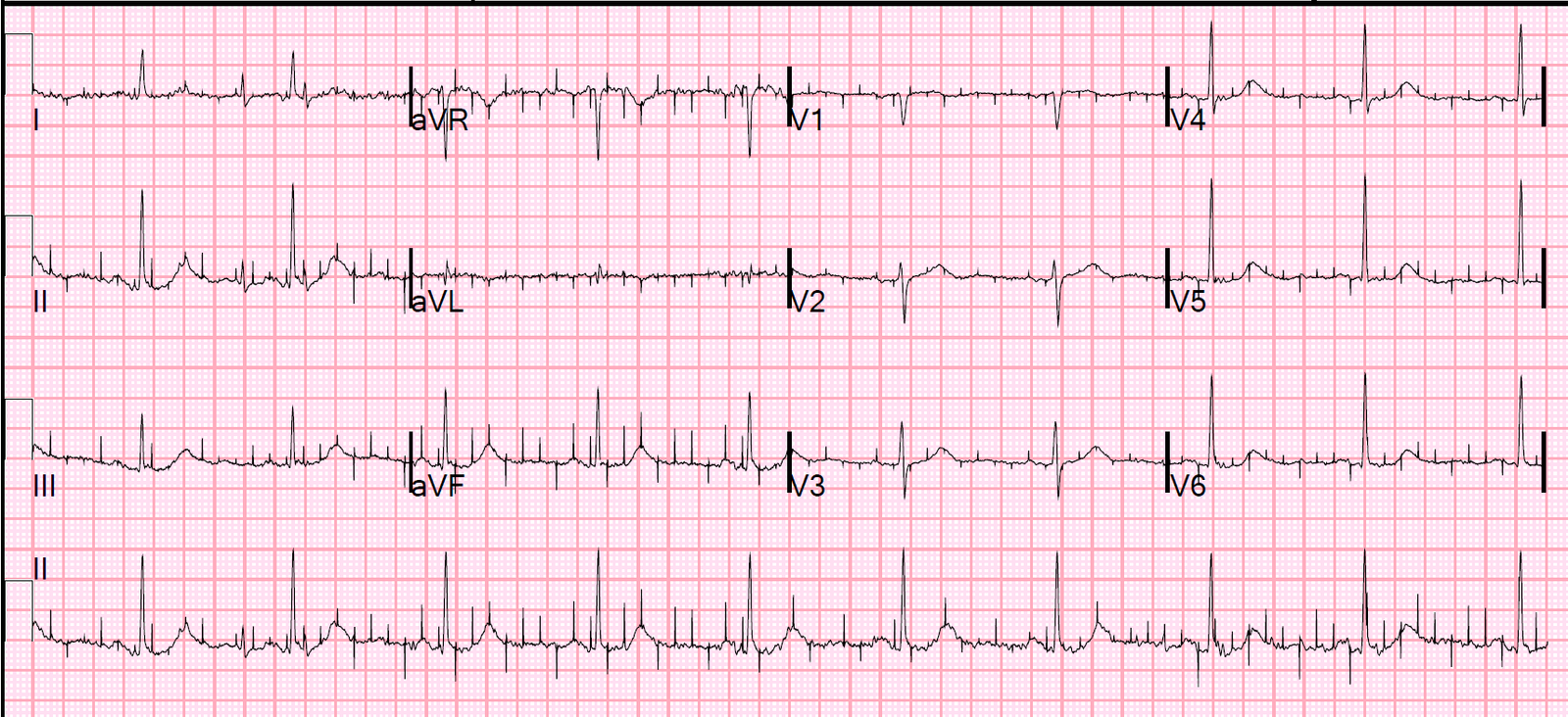
| Sinus tachycardia (NOT VT!). See P-waves in lead II across the bottom.
RBBB and LAFB (wide complex) There is clear STE in aVL, V2, and V3. There is deep reciprocal ST depression in II, III, aVF. |
The cath lab was de-activated. She died of a 100% left main occlusion and peak troponin I of 500 ng/mL (the highest troponin I have ever heard of).
___________________________
Here is another that was missed by the ED providers:
This is a patient with chest pain and the following prehospital ECG:

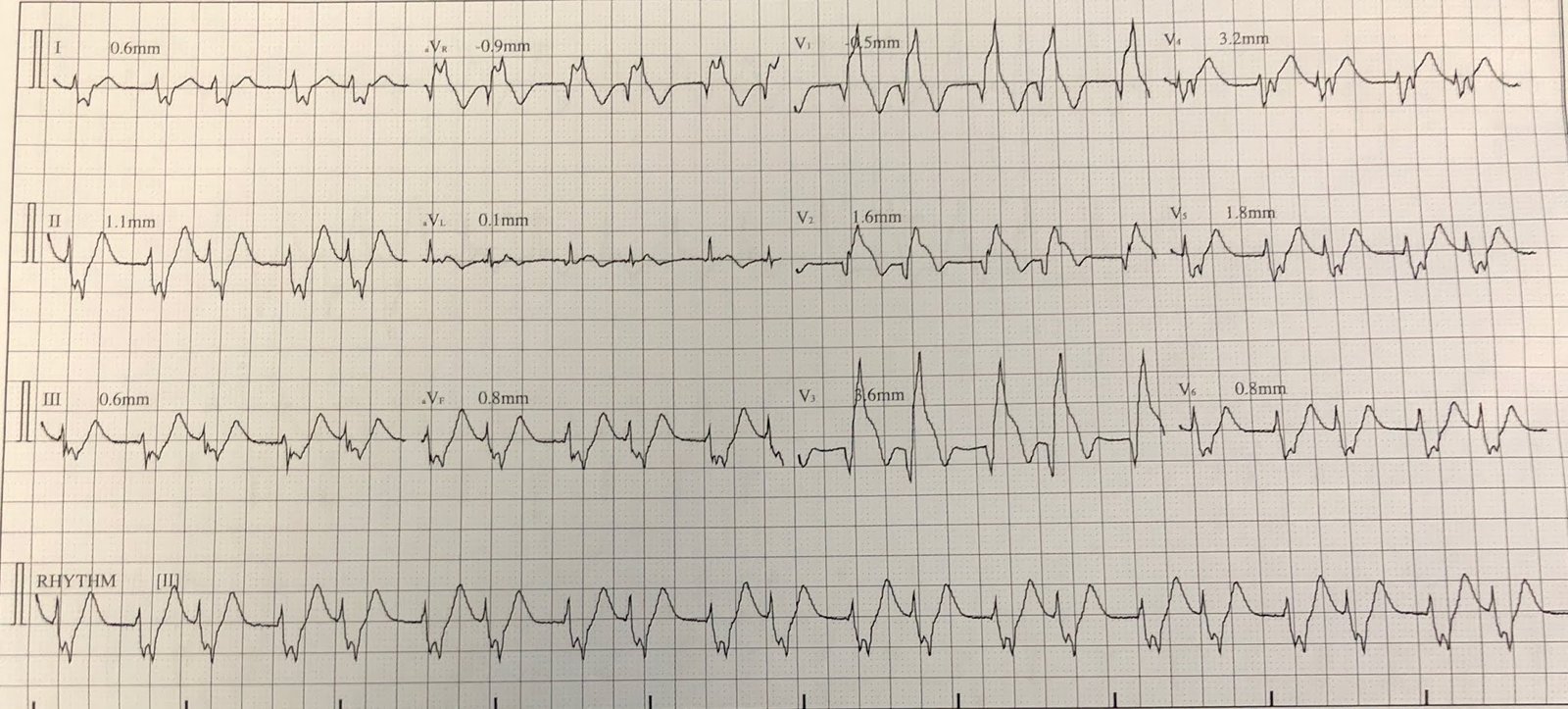
Here are lines that mark the end of the QRS and beginning of the ST segment:
 |
| This also has RBBB and LAFB with ST Elevation, but more subtle This STEMI was not recognized and the patient arrested and could not be resuscitated. |
Learning Points:
1. Level of training does not predict ability to diagnose OMI from the ECG. Paramedics and PA’s can be outstanding at this.
2. Beware RBBB with LAFB. ST Elevation may not be obvious, or it may be. It does distort the ECG and it confuses many ECG interpreters.