I was teaching about subtle coronary occlusion at EKG conference to our residents a couple days ago. About coronary occlusion that does not meet STEMI criteria and that many physicians would miss.
They were asking me about whether, if they missed one of these, would they have missed a STEMI?
I responded:
“No, you would not have missed a STEMI, and you would not be blamed for anything, but you would have missed an opportunity to save the patient’s heart.”
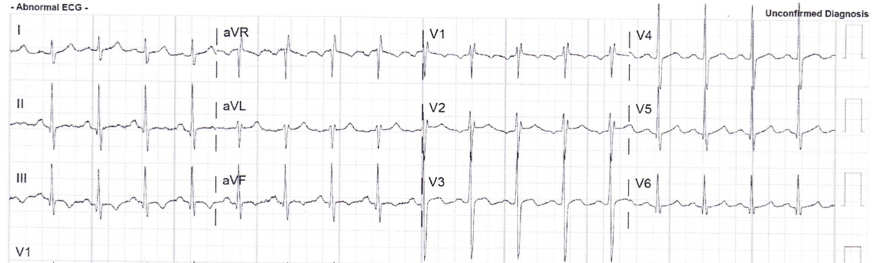
Just as I was explaining this, a text message came through from a former resident, with this ECG and the question: “Diagnostic ECG?”
 |
| What do you think? Notice the computer only sees the inverted P-waves. |
I responded:
“Those are hyperacute T-waves.”
The residents all chimed in: “Do not miss this opportunity!”
So I texted back: “Do not miss this opportunity to save the patient’s heart. It is definitely diagnostic.”
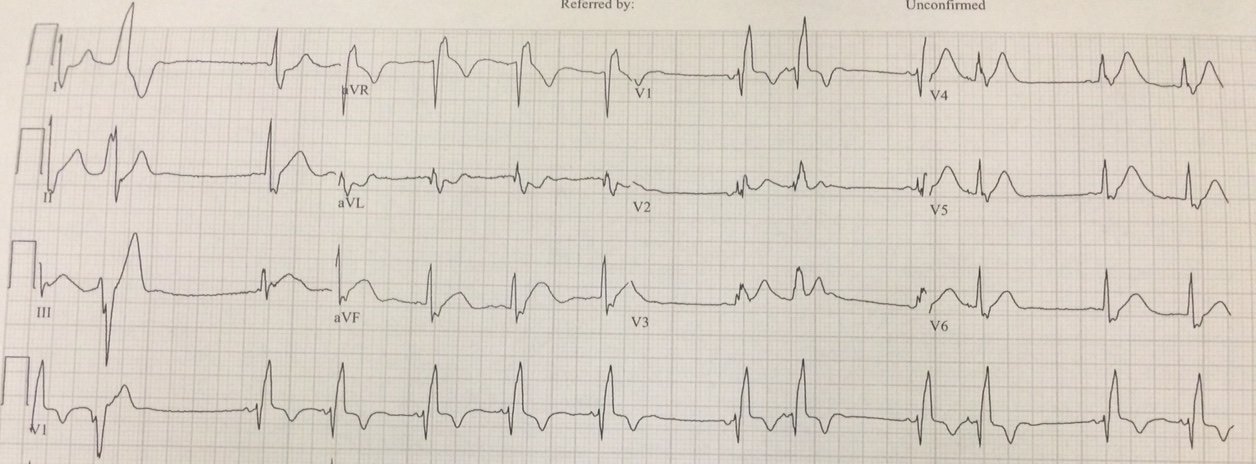
As it turns out, this was a prehospital ECG:
The medics transmitted this to the Emergency physician, asking whether cath lab activation was indicated or not.
The emergency physician diagnosed coronary occlusion (based on the STE in I and aVL, with reciprocal STD in lead III and the hyperacute T-waves in V3-V5).
A cardiologist somehow got involved. He disagreed and said not to activate, and “instead of listening to me,” commenced to “educate me as to why the EKG is normal.”
Comment on ECG:
The pair of leads III and aVL are diagnostic of occlusion.
The hyperacute T-waves in V3 and V4 are diagnostic of occlusion.
The combination is diagnostic of proximal LAD occlusion.
So I asked what the history was, and here it is:
A 60-something man, previously healthy, has sudden CP and diaphoresis. He presented to a clinic where the ECG (not available) was normal and there was a negative single troponin. He was discharged to home from the clinic.
He called 911 for recurrence of pain.
My response was:
“Given the history, you could almost activate the cath lab without an ECG!”
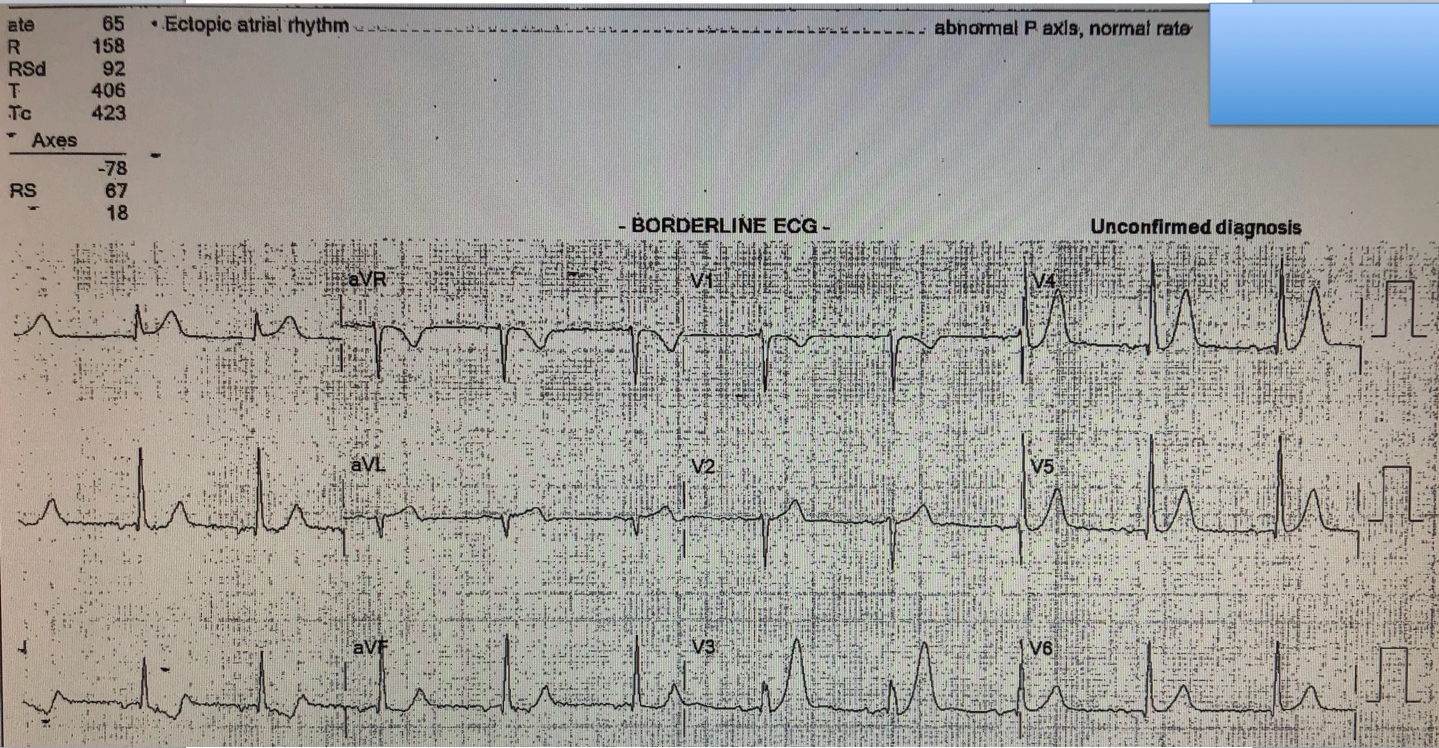
But instead, the emergency physician persisted, and recorded this ED ECG shortly afterwards:
 |
|
|
At angiogram, the proximal LAD was occluded.