A 50-something male ran a 10 mile race, after which he complained of a headache. The next day, he collapsed and had a witnessed seizure.
He arrived agitated and the monitor showed a wide complex tachycardia. He was very hypertensive and tachycardic.
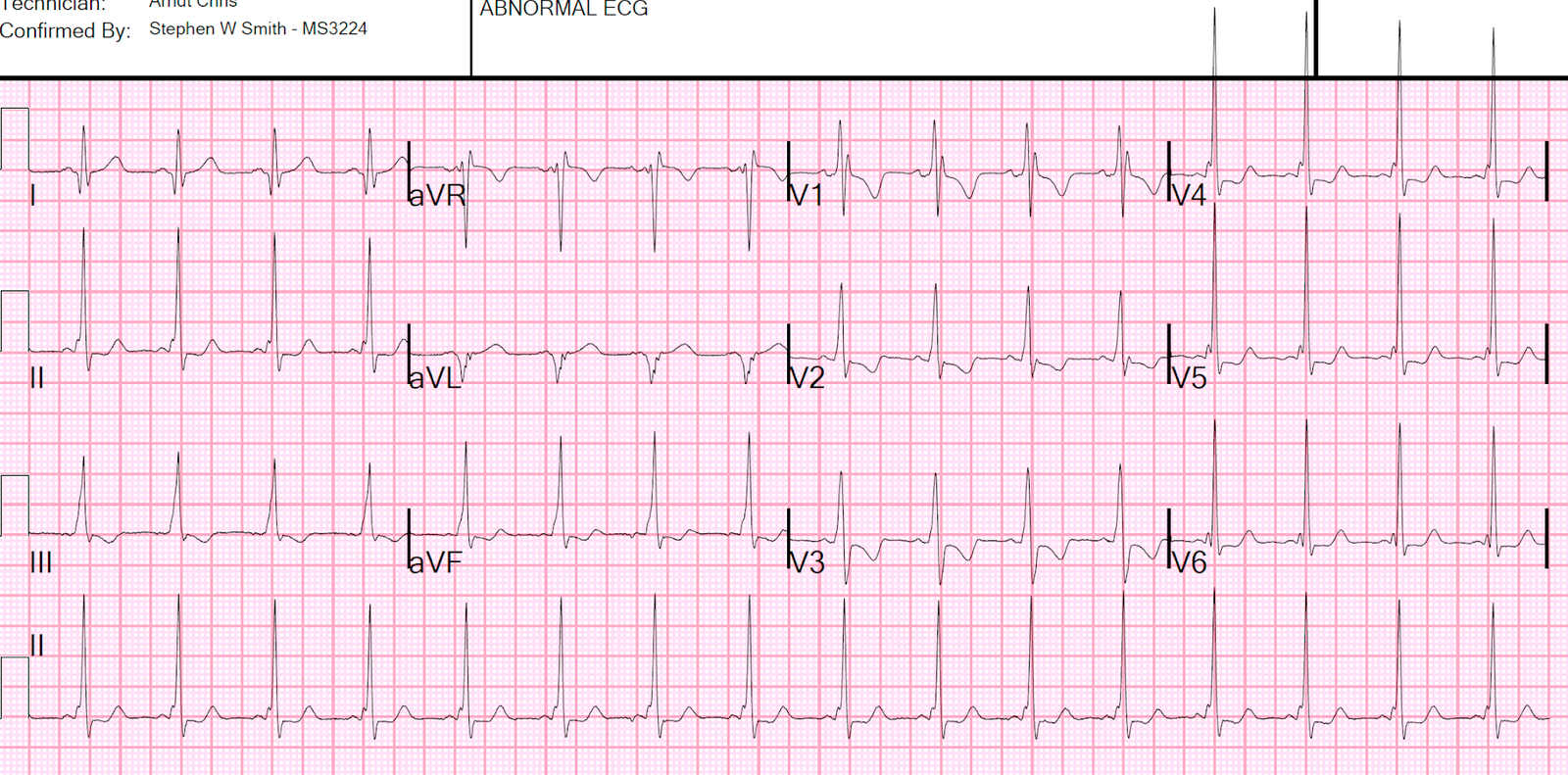
A 12-lead ECG was obtained:

What is it? What therapy?
There are wide complex QRS’s with 2 different morphologies:
1. RBBB configuration with an axis of about 135 degrees (lower right axis toward III)
2. IVCD (neither RBBB nor LBBB) with a “Northwest” (upper right) axis toward aVR
There appear to be 3 possible P-waves, but they are not consistent and not definitely associated with any QRS.
Thus, I thought that this is probably Bidirectional Ventricular Tachycardia.
I sent it to Ken Grauer, and he drew some lines and gave his thoughts:
==============================================

Hi Steve. TRULY interesting — and I’m NOT sure what is going on. My thoughts:
- I don’t see sinus P waves
- The ventricular rhythm looks quite regular. The QRS is wide — and looks to be of ventricular etiology.
- Against
this being bidirectional VT — is that there is a deflection (RED
vertical lines that I drew in V1, V4) that continues precisely on time! I
suspect this may reflect retrograde P waves — and I wouldn’t expect
this to continue if this was bidirectional VT with 2 different
ventricular foci … - I know with VT that the
pathway of VT reentry may vary — that at times part of the pathway may
contain one of the bundle branches — and I suspect that may be what is
intermittently happening here … - P.S. — As in the case of pleomorphic VT that I presented (in the June 1, 2020 post in Dr. Smith’s ECG Blog) — among potential mechanisms for explaining variation between a limited number of QRS morphologies during VT include: i) A single VT circuit with more than a single exit site; ii) More than a single VT circuit; and/or, iii) Shifting conduction properties that alter the activation sequence (Liu & Josephson — Circ Arrhythm Electrophysiol 4:2-4, 2011). — Ken Grauer, MD —
==============================================
With the combination of headache after exertion, followed by sudden collapse with altered mental status, in a previously healthy patient, subarachnoid hemorrhage was strongly suspected. SAH often causes a catecholamine burst and this can result in stress cardiomyopathy (takotsubo), and/or ischemia, with associated VT.
The patient was intubated for his mental status and additionally so that he could be put on a propofol infusion in order to blunt the catecholamine surge, after which the rhythm stabilized.

Sinus tachycardia with some ST depression consistent with subendocardial ischemia
He had a CT scan of the head:

Aneurysmal subarachnoid hemorrhage
Later, a formal echo was done:
The estimated left ventricular ejection fraction is 59%.
Normal estimated left ventricular ejection fraction
Left ventricular hypertrophy concentric
Regional wall motion abnormality-lateral akinetic
Regional wall motion abnormality-anterior akinetic
ADDITIONAL REMARKS
There is definite akinesis of the mid-lateral and basal anterior segments.
(The etiology–i.e. coronary vs noncoronary mechanisms—is unclear on this study).
In combination with elevated troponins (250 ng/mL — NOT high sensitivity), these findings were thought to be due to stress cardiomyopathy (takotsubo).
Learning Points:
1. Learn to recognize Bidirectional VT. See a 2nd case below.
2. Stress cardiomyopathy can be caused by a catecholamine surge, which has many etiologies including Subarachnoid hemorrhage
3. VT can be caused by catecholamine surge in an otherwise relatively healthy heart
4. Propofol has been reported as a treatment for VT caused by catecholamine surge. See search here.
Another case of Bidirectional Ventricular Tachycardia
A Southeast Asian with Tachycardia and Hypotension after taking a dangerous herbal medication (Bidirectional Ventricular Tachycardia from Aconite Poisoning)