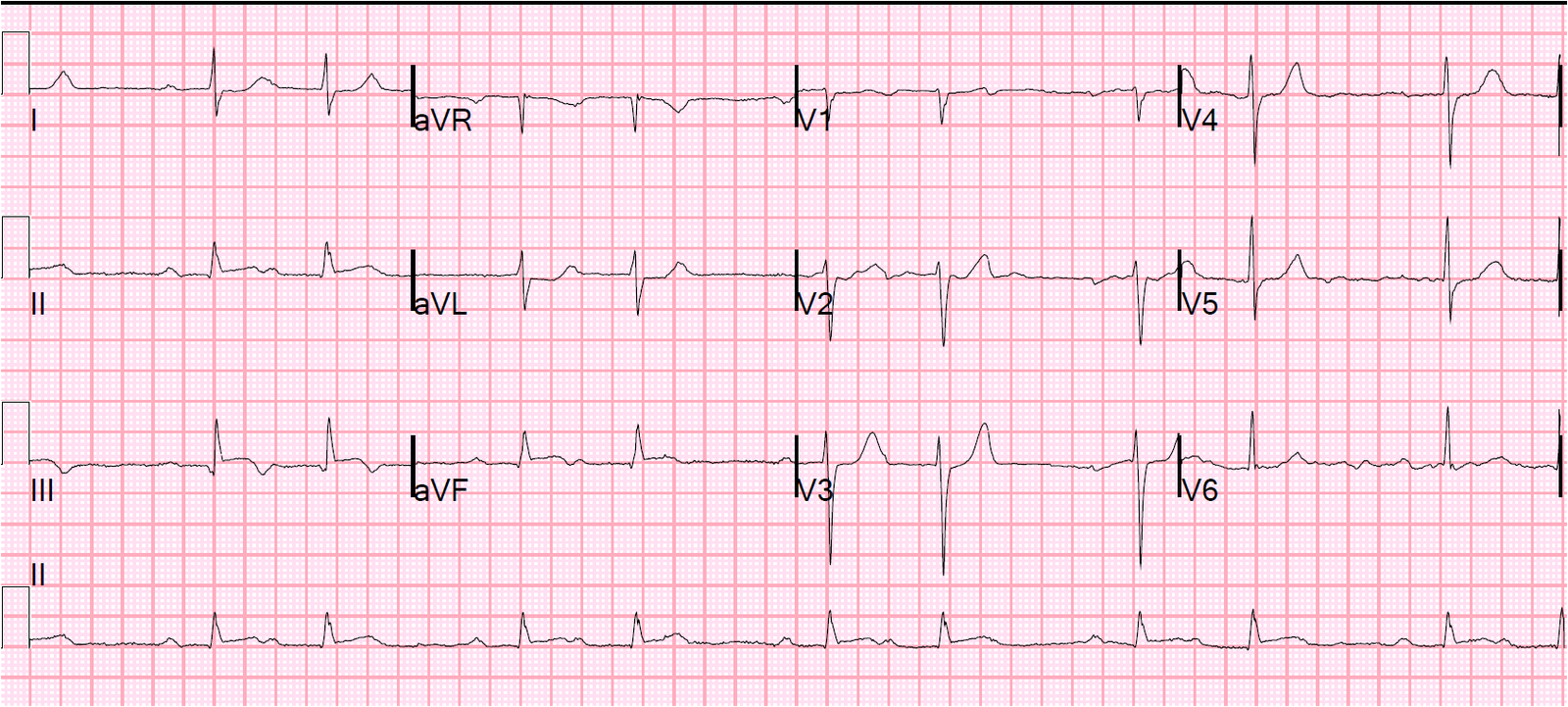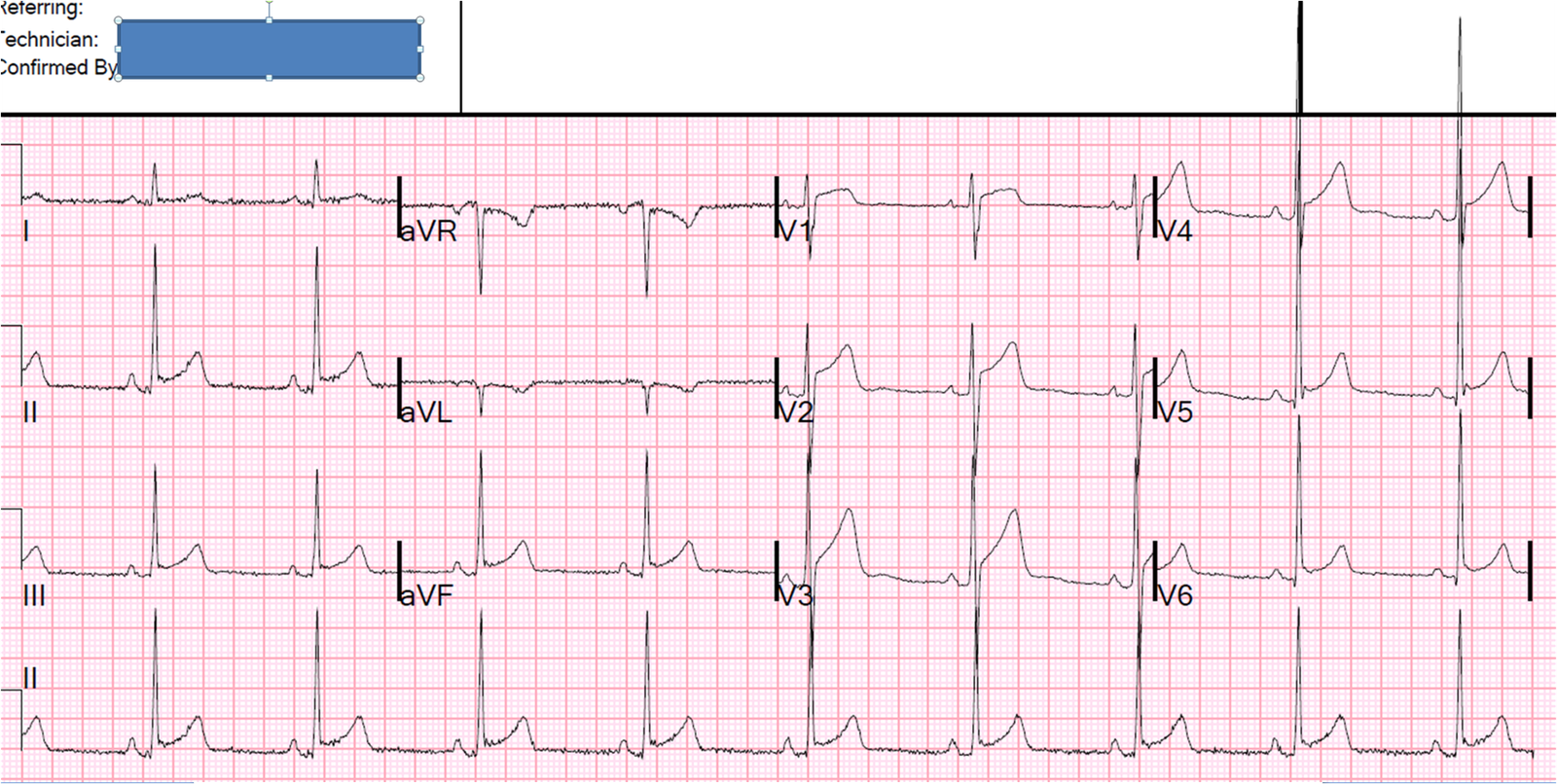
Male in his 40’s with chest pressure: what is the diagnosis
This 40-some year old patient complained of chest pressure and had this ECG recorded: See comments and diagnosis below The providers were a…
Associate Editors:
— Pendell Meyers & Ken Grauer (2018)
— Jesse McLaren & Emre Aslanger (2022)
— Willy Frick (2024) — Sam Ghali (2025)