This is a repost. I’ve received a few questions like this, so wanted to re-inforce the idea of down-up vs. up-down T-waves
Case:
One of our residents texted me this ECG and was worried about Wellens’ waves.
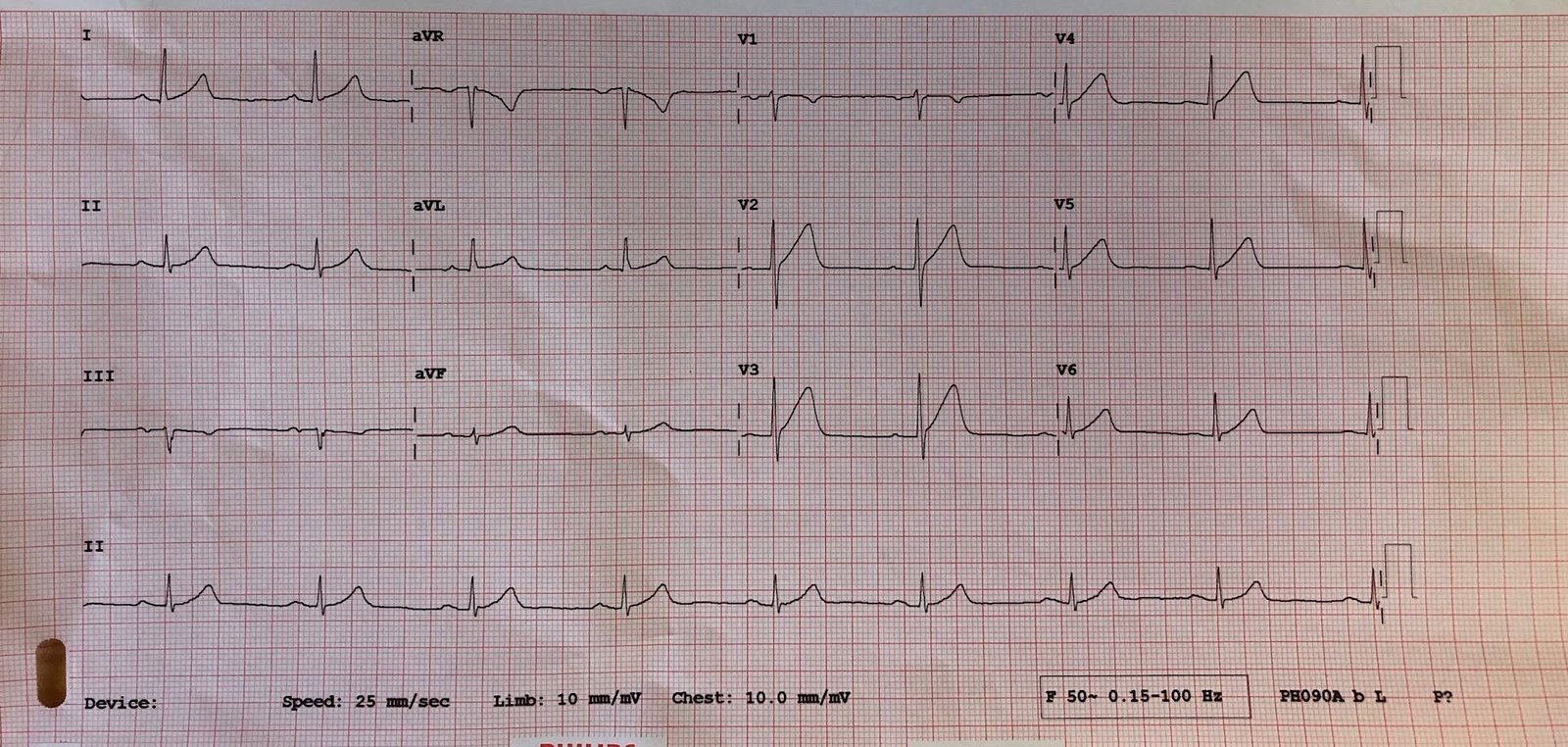
A middle-aged male presented with vomiting. Here was the initial ED ECG:
 |
| What do you think? |
Here is my response: “What is the Potassium?”
Wellen’s waves are always Up-Down T-waves, not Down-Up T-waves as here. Down-Up T-waves in V2 and V3 have only 3 causes, as below.
Moreover, the QT interval is impossibly long at about 560 ms, with a corrected QT of 593 ms (Fridericia correction, which seems to be the best; QTc(Bazett) = 611 ms.
When the QT is impossibly long, think that the “T-wave” is actually a U-wave, not a T-wave.
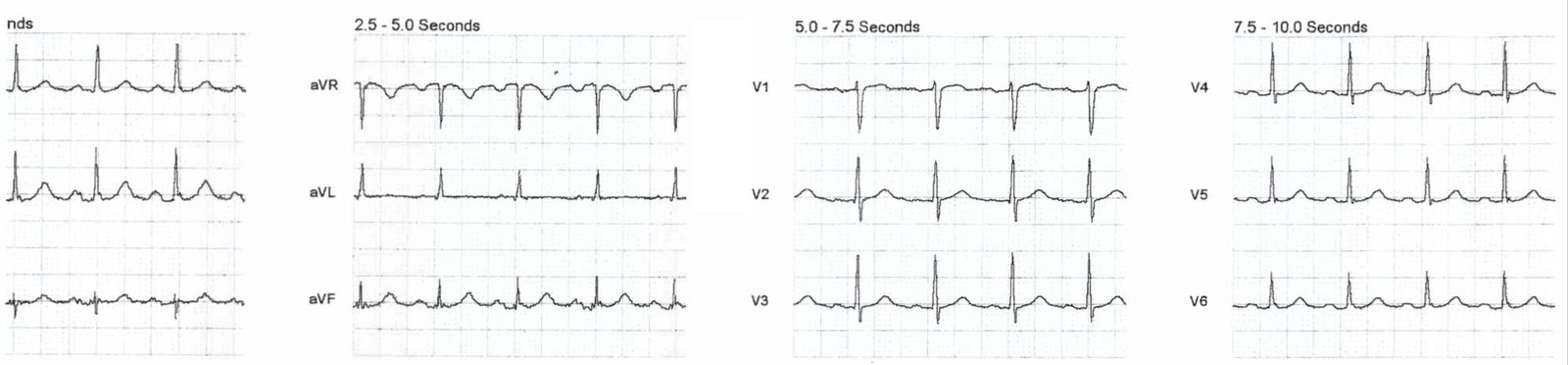
Here the U-waves are highlighted:
 |
| 1. In lead V6, one can discern discrete T-waves (red arrow) and U-waves (black arrow). 2. Go down to rhythm strip lead II across the bottom, identify T- and U-waves there. 3. Go 3 beats earlier in lead II to identify the U-wave there (green line). 4. Draw the green line up to show the U-waves in leads V1-V3 So these are indeed U-waves, not T-waves |
1) Posterior MI with some reperfusion (reciprocal to Up-Down T-waves of the posterior wall, analogous to Wellens’ of the posterior wall as recorded from the anterior wall).
See case below
2) Hypokalemia (in which case the upright component is really a U-wave). In this case, V6 is pathognomonic: you can see a clear large U-wave following the T-wave. It must be hypokalemia. Notice also the very long QT, which is really a long QU-wave.
Other down-up T-waves:
3) Reciprocal findings between leads III and aVL in post-ischemic (Wellens’ type) T-waves:
In lead III: reciprocal to up-down (Wellens’ type) post-ischemic T-waves in aVL.
In lead aVL: reciprocal to up-down (Wellens’ type) post-ischemic T-waves in III.
The K was 2.0 mEq/L.
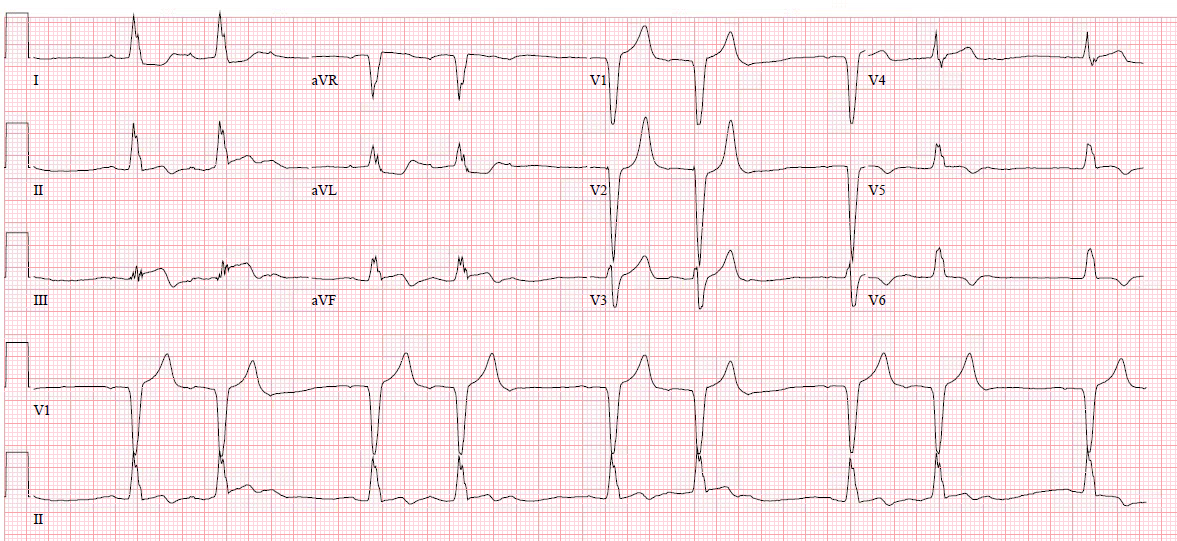
For contrast: Here are classic Wellens Pattern A (biphasic) waves:
 |
|
Clinical Course
Here, again, the previous ECG at K = 2.0 mEq/L:
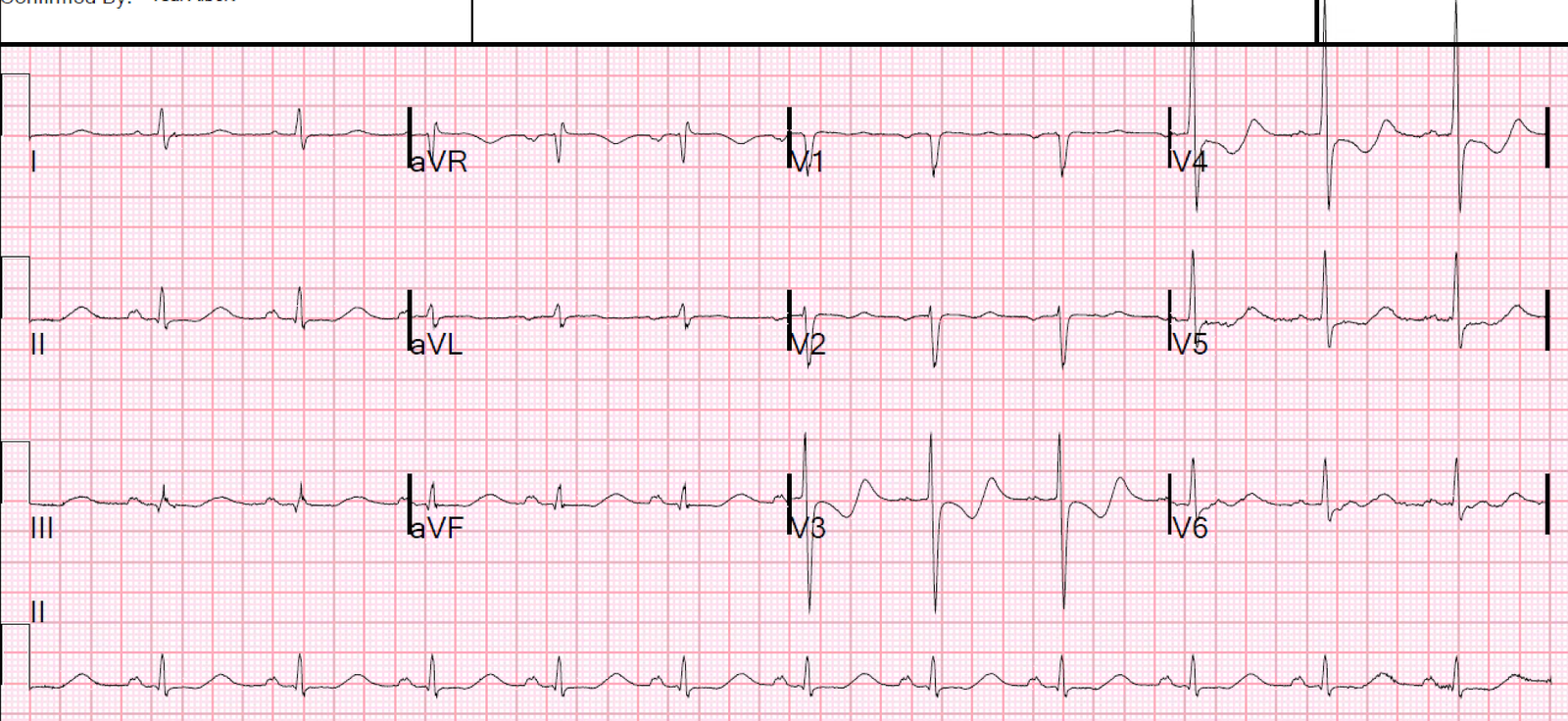
Here is an example of a Down-Up T-wave from Reperfusing Posterior MI. Series of Prehospital ECGs Showing Reperfusion of Inferior-posterior STEMI:
See this too: Classic Evolution of Wellens’ T-waves over 26 hours
Learning Points
(Pattern B is deep symmetric inversion) |