Thursday’s case, read by 60,000 people, provoked a bit of anguish among readers because they weren’t all sure they would recognize this finding of LAD occlusion. Others thought it was obvious. Others thought they would detect it with troponins or serial EKGs (serial EKG was done and did not change; I don’t know about serial trops, but one was “negative.”) Some persistently denied that the T-wave in V2 was a specific sign of ischemia.
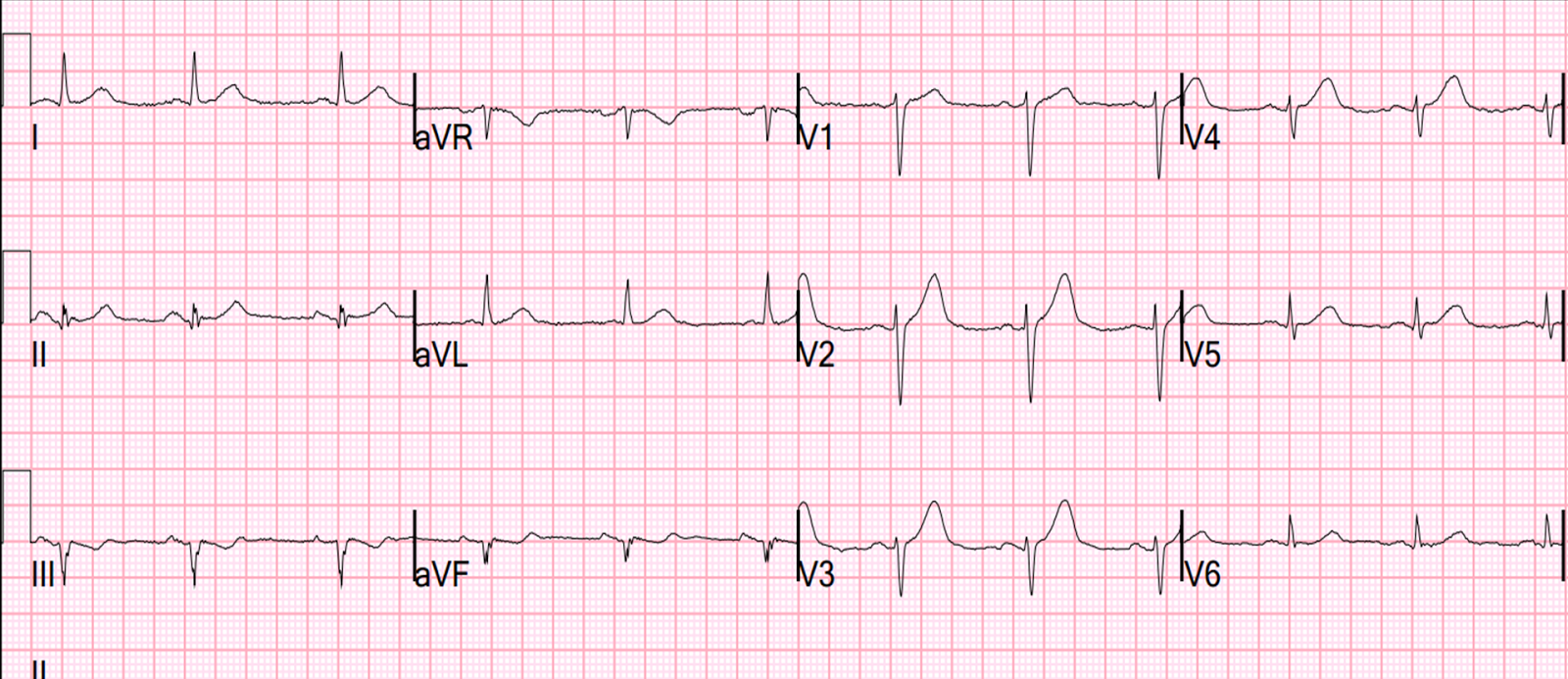
These are 10 cases of LAD occlusion with subtle Hyperacute T-waves in lead V2 (or V3) only.
Steps to verify LAD occlusion, or exclude it:
1. Use of the LAD occlusion/early repolarization formula. But beware the few false negatives, especially when there are hyperacute T-waves but no ST elevation (see Case 2 below):
Formula to differentiate Normal Variant ST Elevation (Early Repolarization) from Anterior STEMI.
2. Use contrast echocardiography (This is the most reliable, short of angiography). Bedside echo without contrast or speckle tracking can be misleading. You must be an expert at this to rule out a wall motion abnormality.
Looking for a wall motion abnormality with bedside echo can lead you astray
3. A positive troponin is useful. A negative one does not rule out MI. 2 or 3 do not rule out unstable angina, even in the era of high sensitivity troponin: this study by Thelin et al. showed 100% sensitivity for MI, but only 95% sensitivity for ACS using hs-TnT.
4. Angiography.
Ten (10) Cases of Acute LAD occlusion manifesting as subtle hyperacute T-waves
Case 1
https://drsmithsecgblog.com/2013/06/a-tough-ecg-but-learn-from-it.html
Case 2

https://drsmithsecgblog.com/2010/08/35-yo-woman-with-lad-occlusion.html
Case 3 (April 20 case that provoked this post)

https://drsmithsecgblog.com/2016/04/a-37-year-old-woman-with-chest-pain.html
Case 4

https://drsmithsecgblog.com/2015/04/a-very-subtle-lad-occlusiont-wave-in-v1.html
Case 5

https://drsmithsecgblog.com/2016/03/this-case-was-sent-by-one-of-our-great.html
Case 6

https://drsmithsecgblog.com/2015/10/a-40-something-with-chest-pain.html
Case 7 (this one links to many other cases of hyperacute T-waves.

https://drsmithsecgblog.com/2014/04/chest-pain.html
Case 8

https://drsmithsecgblog.com/2011/07/missed-stemi-spontaneously-reperfused.html
Case 9

https://drsmithsecgblog.com/2014/12/i-was-reading-stack-of-ecgs-yesterday.html
Case 10
 |
| This one is not posted, but was an LAD occlusion that went unrecognized. The patient lived but lost the entire anterior wall. |
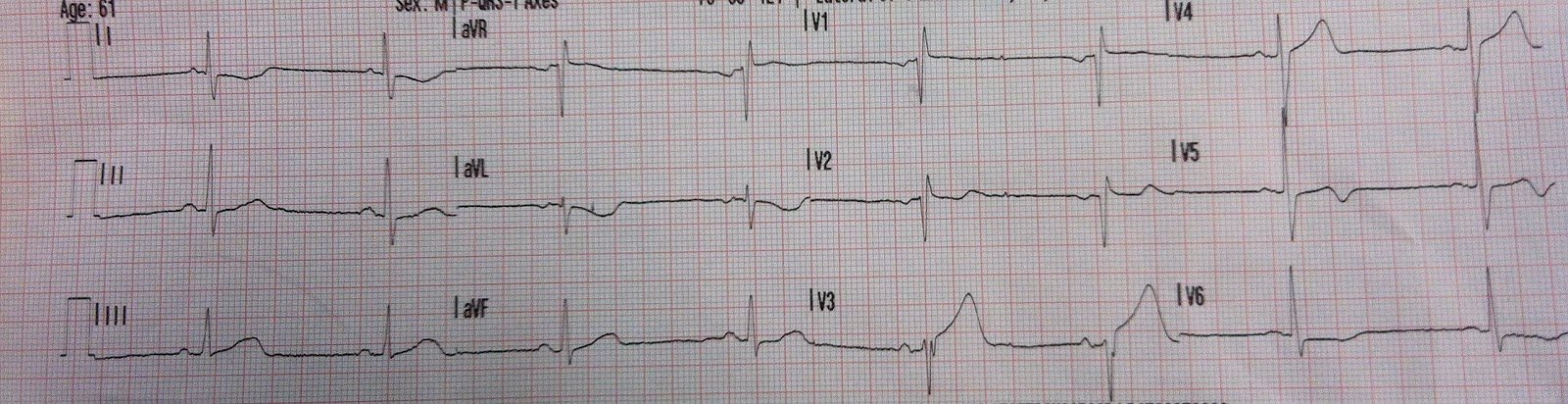
Case 11.
A 20-something presented with one hour of chest pain.
This is from Sweden, where they record at 50mm/sec. Therefore, I compressed the grid so it would look like a standard ECG:
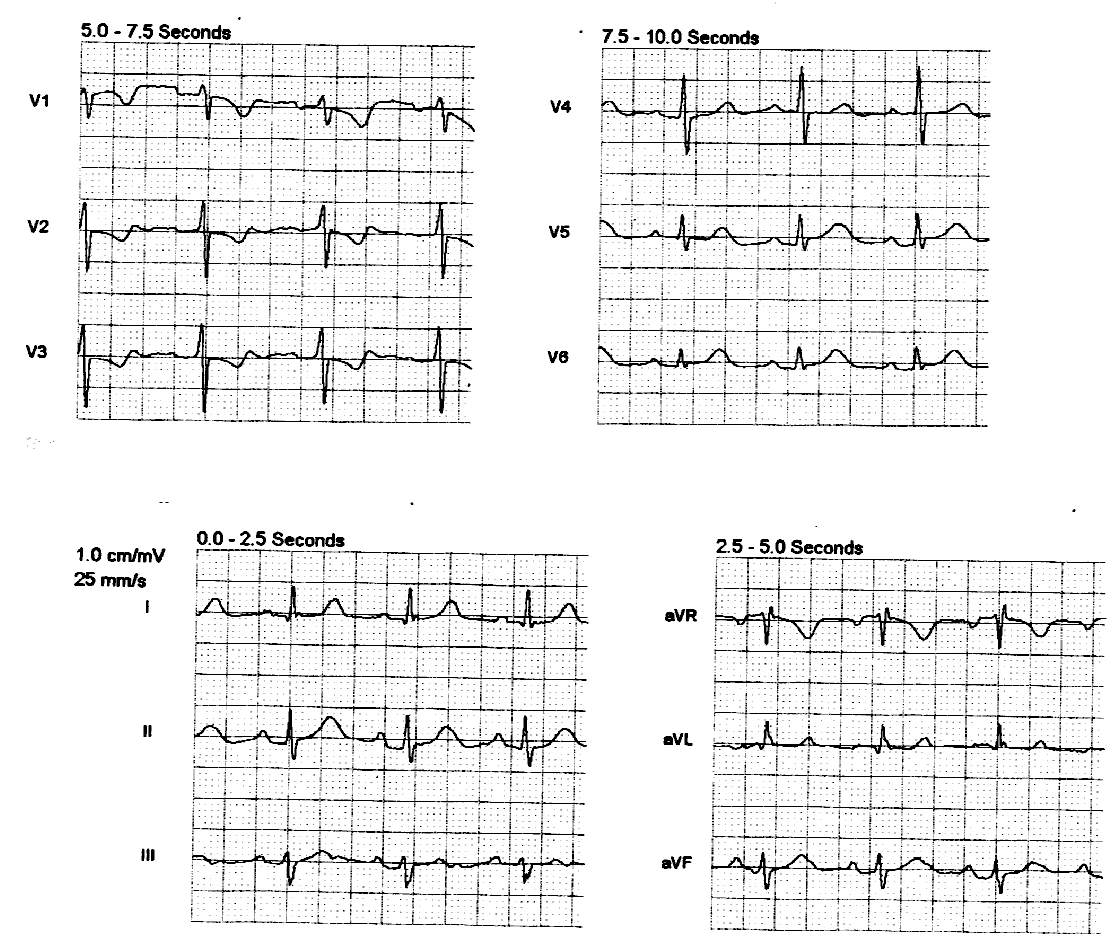
 |
| At t = 17 minutes, the T-waves are larger |
Here the two tracings are superimposed on each other:
 |
| You can see the larger size of the T-waves on the second ECG. |
The high sensitivity troponin T was 5 ng/L (barely measurable: LoD = 5 ng/mL, 99% = 14 ng/mL.
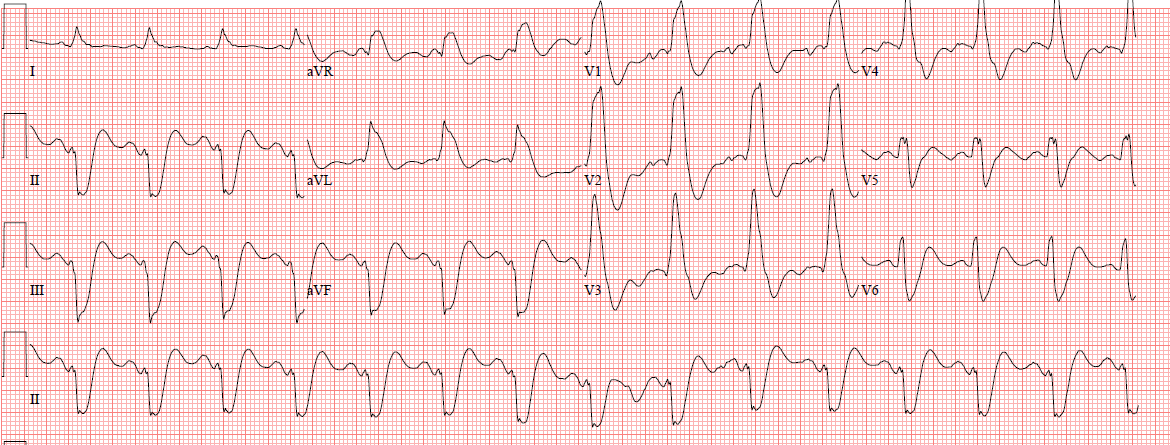
This was missed.
The next ECG was 2.5 hours later and showed a huge anterolateral STEMI.