A middle-aged male presented with “burning” mid chest pain, with radiation to bilateral shoulders (pain radiating to both shoulder is very specific for ischemia). It started about 5 hours prior to arrival. He obtained little relief from nitro x 3 by EMS. There was a history of previous MI, with a stent in the 1st Obtuse Marginal. He had taken his Plavix for 6 months, then discontinued and also stopped taking his antihypertensives and statin. He continued to smoke about 1.5 pks per day.
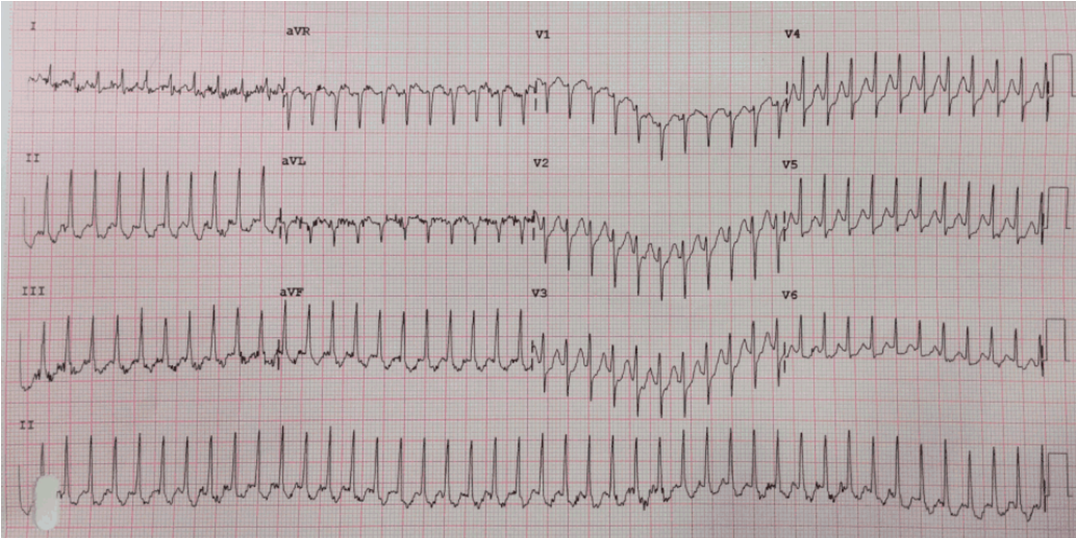
Here is his ECG:
 |
| Junctional Bradycardia (this is sinus arrest with junctional escape, and is highly suggestive of ischemia).
There is a pathologic Q-wave in lead III (old? new?). There is slight ST depression in leads I, II, and V3-V6 (fairly specific for ischemia). Down-Up T-wave in aVL: very specific for ischemia! There are slightly hyperacute T-waves in inferior leads (probable ischemia). |
These are subtle findings. No single finding is diagnostic of ischemia but he has a very specific combination of factors:
1. typical pain
2. h/o coronary disease
3. pain radiating to both shoulders
4. junctional bradycardia
5. Q-waves
6. ST depression
7. Down-Up T-wave in aVL
7. Possible hyperacute T-waves
All of these together, but none of them by themselves, diagnose acute MI.
One of my former residents diagnosed this as inferior MI and activated the cath lab. I love it when my residents become better than I at reading ECGs!
There was a 100% acute occlusion of the RCA, with ischemia of the SA node causing sinus arrest.
Lesson:
1. When highly suggestive ECG signs of ischemia combine with a high pretest probability and refractory ischemic pain, activate the cath lab even if the ECG does not meet STEMI criteria.