This was sent by a former resident:
- A 40-something previously healthy and “very fit” woman presented to a small hospital without PCI capability.
Aside: the worst thing you can be if you have an MI is a young woman. A couple other cases:
- 30-something woman with a HEART score of zero, EDACS of 2, computer “Normal” ECG, and initial troponin < Limit of Detection
- The worst thing you can be when you have this ECG is to be a young woman
= = =
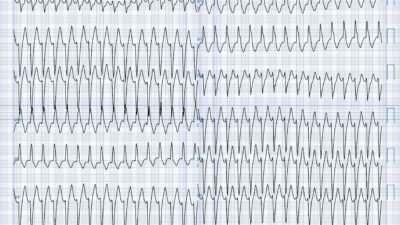
Today’s patient presented after a few days of intermittent chest burning, now with constant “intense” chest burning. There is no mention of dyspnea. This ECG was recorded during pain:
— What do you think? —
= = =
= = =
This was sent to me and, although there is diffuse ST depression and T-wave inversion which suggests diffuse subendocardial ischemia, I don’t see evidence of total OMI. Nevertheless, I texted back that “due to an ischemic ECG with constant chest pain, the patient needs the cath lab now.”
The Queen of Hearts does not see OMI either.
= = =
Waxing and waning burning pain that then becomes constant is extremely typical for ACS/OMI, and absence of dyspnea would be unusual in pulmonary embolism (PE).
However, tachycardia is unusual in ACS unless there is cardiogenic shock, or impending shock. So it is reasonable to investigate pulmonary embolism. So they did a CT pulmonary angiogram.
- It was negative for PE, but it showed ischemic myocardium:
Interpretation: There are areas of the subendocardium which are hypoperfused (dark, contrast is not getting there ==> ischemic).
= = =
Case Continued:
The first hs troponin (I or T? — doesn’t matter) — was “in the 100s”
The MD at the small hospital activated the cath lab at the referral center. The referral center responded that it does not meet their criteria for emergent cath lab activation.
- She was transferred to the referral hospital on heparin with a diagnosis of “NSTEMI” (a worthless diagnosis) and scheduled for next day cath.
Smith: Even if you don’t believe the ECG is ischemic (which it surely is) — this elevated troponin definitively establishes acute MI in a patient with no previous cardiac history. Such a patient with persistent chest pain must go emergently to the cath lab! The ACC/AHA guidelines mandate this, but it is only followed 6% of the time!
- Before she got to cath, she arrested and required ECMO. Angiogram showed 100% LAD occlusion (I don’t know if proximal or mid). I’m not sure if she survived.
= = =
My former resident writes:
- “My experience with cardiologists (almost universally) for EKGs that do not classically fit STEMI, or incompletely meet their cath requirements — is that there is a big delay. When I reiterate my concerns or show what I see as evidence of poor perfusion (like the CT above), there is resistance. I need to learn how to better speak their language.”
= = =
This is a case in which their own guidelines would say the patient must go emergently to the Cath Lab. But the literature shows that cardiologists follow this guideline 6% of the time.
- [Lupu L, Taha L, Banai A, et al. Immediate and early percutaneous coronary intervention in very high-risk and high-risk non-ST segment elevation myocardial infarction patients.
- Clin Cardiol [Internet] 2022;Available from: https://onlinelibrary.wiley.com/doi/10.1002/clc.23781].)
Moreover, the guidelines, which are for “high risk” NSTEMI, mostly depend on a troponin diagnosis of MI (NSTEMI), or a very high clinical suspicion. They do not rely on subtle ECG interpretation of occlusion, which would lead to very fast reperfusion and best chance of a good outcome.
= = =
======================================
MY Comment, by KEN GRAUER, MD (3/6/2026):
Reviewing cases “on paper” after the fact is not an easy task. Not having been at the scene where the patient presented for medical care — we often lack key information that is difficult (if not impossible) to resurrect from review of the paper chart.
- My comments below reflect the above perspective.
= = =
Regarding Today’s CASE:
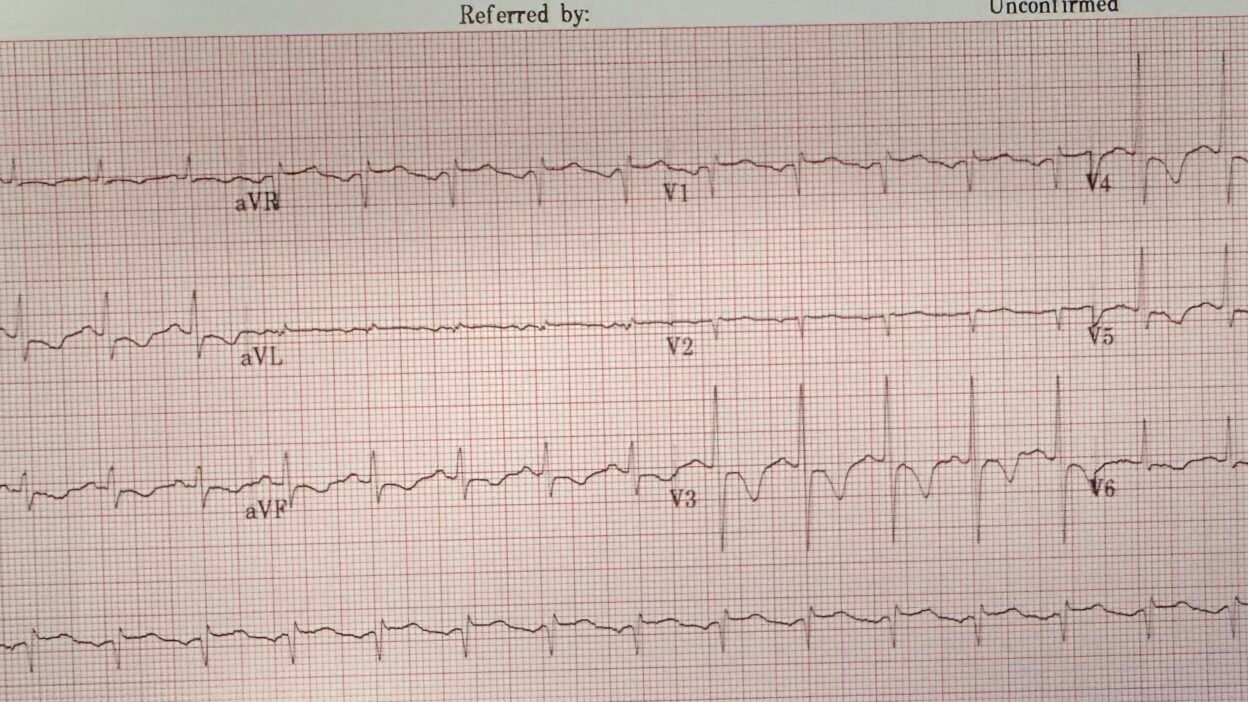
I received the ECG in Figure-1 — and learned it was from a 40-something previously healthy woman who presented with several days of “chest burning”. She noted “intense chest burning” at the time this initial ECG was recorded.
- To Emphasize: There are many details about today’s case regarding what happened when, and under what clinical circumstances — that we just do not know about. As a result — my comments are not directed at either the cardiology or emergency team that took over management of this patient — but instead, merely reflect My Thoughts on how I might approach this case with the limited information we are given (without necessarily knowing if the sequence of actions I suggest were undertaken).
- For Example: Today’s patient presented with a relatively fast sinus tachycardia. Yet there is no mention from the information we are given as to Why this patient might be in a rapid sinus tachycardia, which is a relatively uncommon cardiac rhythm in an uncomplicated acute MI (ie, No vital signs or pertinent exam findings are provided — there is no indication of the patient’s blood pressure or respiratory rate — and no mention of possible heart failure or pulmonary compromise).
- KEY Point: Whatever approach is taken toward evaluating this patient should aim as soon as is possible to uncover the cause of the sinus tachycardia.
= = =
My Interpretation of ECG #1 given the above History:
- As noted above — the rhythm of the ECG in Figure-1 is sinus tachycardia at ~115/minute.
- Regarding intervals — the PR interval is normal and the QRS is narrow. Considering the rapid rate — the QTc is at least borderline prolonged.
- The frontal plane axis is normal (at about +60 degrees).
- There is no chamber enlargement.
- NOTE: I suspect that the lead V1 (and probably also lead V2) electrodes have been placed too high on the chest because: i) There is an r’ complex in lead V1 in this patient without other real sign of incomplete RBBB (only the tiniest terminal s wave is seen in lateral leads I,V6); — ii) The P wave in lead V1 is entirely negative (with a hint of a negative P wave also in V2); — iii) QRST morphology in lead V1 looks identical to the QRST complex in lead aVR; — and, iv) The tiny QRS in lead V2 simply looks “out of place” — as it is sandwiched in between the Qr complex in lead V1 — and the surprisingly large R=S wave complex with deep negative T wave that so abruptly appears in lead V3 (See the ADDENDUM below for more on how to quickly recognize too high placement of the V1,V2 electrodes — as well as this LINK to the upper Menu in every page in Dr. Smith’s ECG Blog for more examples of V1,V2 misplacement and other “Technical “Misadventures”).
- KEY Point: As I’ll discuss momentarily — the fact that the lead V1,V2 electrodes are probably misplaced is clinically relevant for optimal interpretation of today’s ECG!
Regarding ST-T Wave Changes in Figure-1:
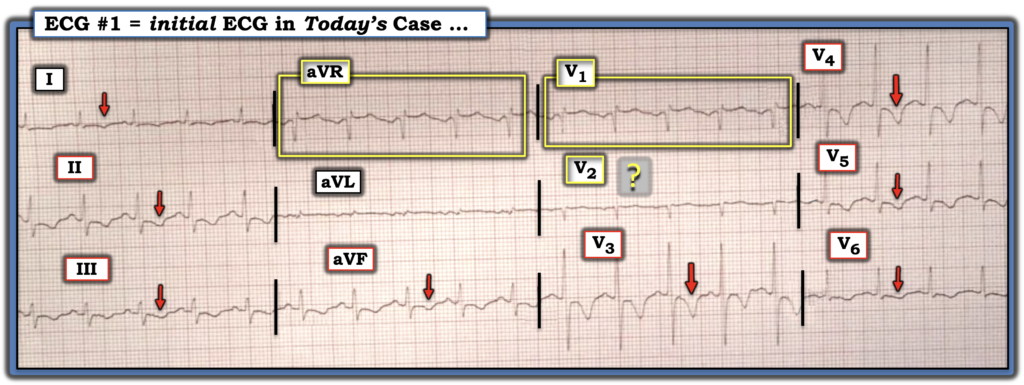
- There is diffuse symmetric T wave inversion in today’s ECG (RED arrows in Figure-1). These T waves are especially deep in anterior leads V3,V4.
- And — We do not know if there might also be T wave inversion beginning as early as in leads V1,V2 — because the V1,V2 electrodes are most probably improperly placed.
= = =
Figure-1: The ECG in today’s case — recorded from a 40s woman during “intense chest burning”.
= = =
My Impression of Today’s ECG in Figure-1:
From a pure ECG interpretation standpoint — I was uncertain if the tracing in Figure-1 was more suggestive of an acute ischemic process — or — of a large acute PE (Pulmonary Embolus).
- The diffuse T wave inversion with ST elevation in lead aVR could be consistent with DSI (Diffuse Subendocardial Ischemia) — or even reperfusion T waves following LAD OMI.
- On the other hand — inferior and anterior T wave inversion in this patient with sinus tachycardia might represent the RV “strain” of a patient with a large acute PE (even though the only symptom cited in the history that was given is “intense chest burning” — and even though the T wave inversion extends out to lateral leads I and V6, which is less commonly seen with RV “strain”).
- And — We do not know if there might also be T wave inversion beginning as early as in leads V1,V2 — because the V1,V2 electrodes are most probably improperly placed.
= = =
The Course of Events:
- Today’s patient was initially seen at a small outlying hospital. On the basis of the initial ECG — the cath lab was activated (with this cath to be performed once the patient arrived at the referral hospital). That said — clinicians at the referral hospital then apparently changed their mind and refused to do emergency cath because this initial ECG “did not meet emergency cath lab activation criteria”. They instead deferred cardiac cath until the next day.
- The 1st Troponin came back “in the hundreds”.
- Concern at the small outlying hospital about a possible acute PE was apparently great enough — that time was spent performing a CT pulmonary angiogram before transferring the patient to the referral hospital.
- And then, before the next day cath could be performed at the referral hospital — the patient suffered a cardiopulmonary arrest.
- Unfortunately — We lack further follow-up . . .
= = =
Simple Things to Do along the Way:
Admittedly viewing today’s case in the “retrospectoscope” (with my full acknowledgment that much clinical information is lacking) — it seems that the main differential diagnosis was between an acute ischemic process — vs — a large acute PE.
- Time was critical. Potentially — Bedside Echo performed by a skilled operator could have told us within minutes (long before results returned from the CT pulmonary angiogram) — whether the RV was dilated. If dilated — then we would know within minutes that we are almost certainly dealing with a large acute PE.
- And if the marked, diffuse T wave inversion with sinus tachycardia was the result of an acute PE — these ECG findings would then strongly suggest that this acute PE is submassive or massive (lesser PEs rarely produce diffuse RV “strain” with such tachycardia).
- If instead, the marked chest lead T wave inversion was from acute LAD occlusion — Bedside Echo might have quickly given us this answer by revealing a localized wall motion abnormality.
- But even before bedside Echo is performed — a brief physical exam of the patient may have been insightful. If this patient was not tachypneic — then we would know within seconds that the patient is highly unlikely to have a submassive or massive acute PE.
- NOTE: The most commonly omitted vital sign in my experience — is the recording of an accurate respiratory rate. At least 20 seconds by the treating clinician (not copying the nursing notes) — need to be spent looking at the patient to ensure an accurate count of how fast the patient is breathing (and not simply writing 12-15/minute). Over the years — I’ve been amazed at how quietly patients can be breathing at a respiratory rate of over 30/minute (which in today’s case — would be critical data consistent with an acute PE or heart failure).
- Bottom Line: As soon as bedside Echo makes submassive or massive PE unlikely (which should be accomplished within minutes) — We are left with an acutely ischemic ECG in a patient with worrisome tachycardia — an initial Troponin “in the hundreds” — and a patient with persistent symptoms of “intense chest burning”. This patient needs the cath lab.
= = =
= = =
Addendum: Recognizing V1,V2 Misplacement …
Despite an alarming frequency of lead placement errors — the “good news” is that it is EASY to suspect when misplacement of leads V1/V2 is likely! There are 3 Clues to look for:
Suspect leads V1 and/or V2 have been placed 1 or 2 interspaces too high on the chest IF one or more of the following clues are present:
- Clue #1 — If there is an r’ in leads V1 and/or V2, especially if the other finding for incomplete RBBB (ie, terminal s waves in lateral leads I and V6) is absent.
- Clue #2 — If there is a significant negative component to the P wave in lead V1 and/or V2.
- Clue #3 — If the appearance of the P wave, QRS complex and ST-T wave in leads V1 and V2 looks very much like the P wave, QRS complex and ST-T wave in lead aVR.
NOTE: As helpful as the above 3 Clues are for quickly suspecting too high placement of leads V1 and/or V2 — these clues are not infallible. There are times when despite our suspicion from looking at an ECG that leads V1 and V2 have been placed too high — this will turn out not to be the case. For example: i) Incomplete RBBB may truly be present (resulting in a terminal r’ in leads V1 and/or V2); — ii) An all negative, relatively large P wave may sometimes be seen in leads V1,V2 as a normal finding — or — the patient may have true left atrial enlargement; — iii) Variation in body habitus and chest wall anatomy may produce unusual ECG findings; —and/or — iv) The patient may truly have had prior septal infarction.
- Therefore, my goal in presenting these 3 clues — is that they suggest when to suspect that an unusual anterior lead appearance might best by explained by too-high positioning of lead V1 and/or V2.
- It’s EASY to check out your suspicion. Simply verify that chest lead placement is correct — and then REPEAT the ECG!
= = =
= = =