A 32 year old woman with chest pain has a prehospital ECG:
 |
| What do you think?
Is it really “due to ventricular hypertrophy,” as the computer says? |
This was texted to me and my response was:
“Leads are reversed. Correct them and I think you will find a STEMI (or OMI). Either inferoposterior or posterolateral.”
Analysis:
The QRS is negative in I, II, and aVL and positive in aVR, all of which makes for a bizarre axis. Normally you can determine if it is truly lead placement by looking at P-waves, which should be upright in lead II. Here it is difficult to see them. But another way is to see if the QRS is negative in the lateral precordial leads. Here the QRS is positive.
This could also be seen if a right sided ECG is recorded in someone with dextrocardia (this would be extremely unusual!)
There is ST Elevation in aVR and STD in I, II, and aVL. Clearly there should be ST Elevation in lateral leads and ST depression in the right sided lead aVR.
I believe that the right and left arm leads are reversed, but in any case lead reversal is certain.
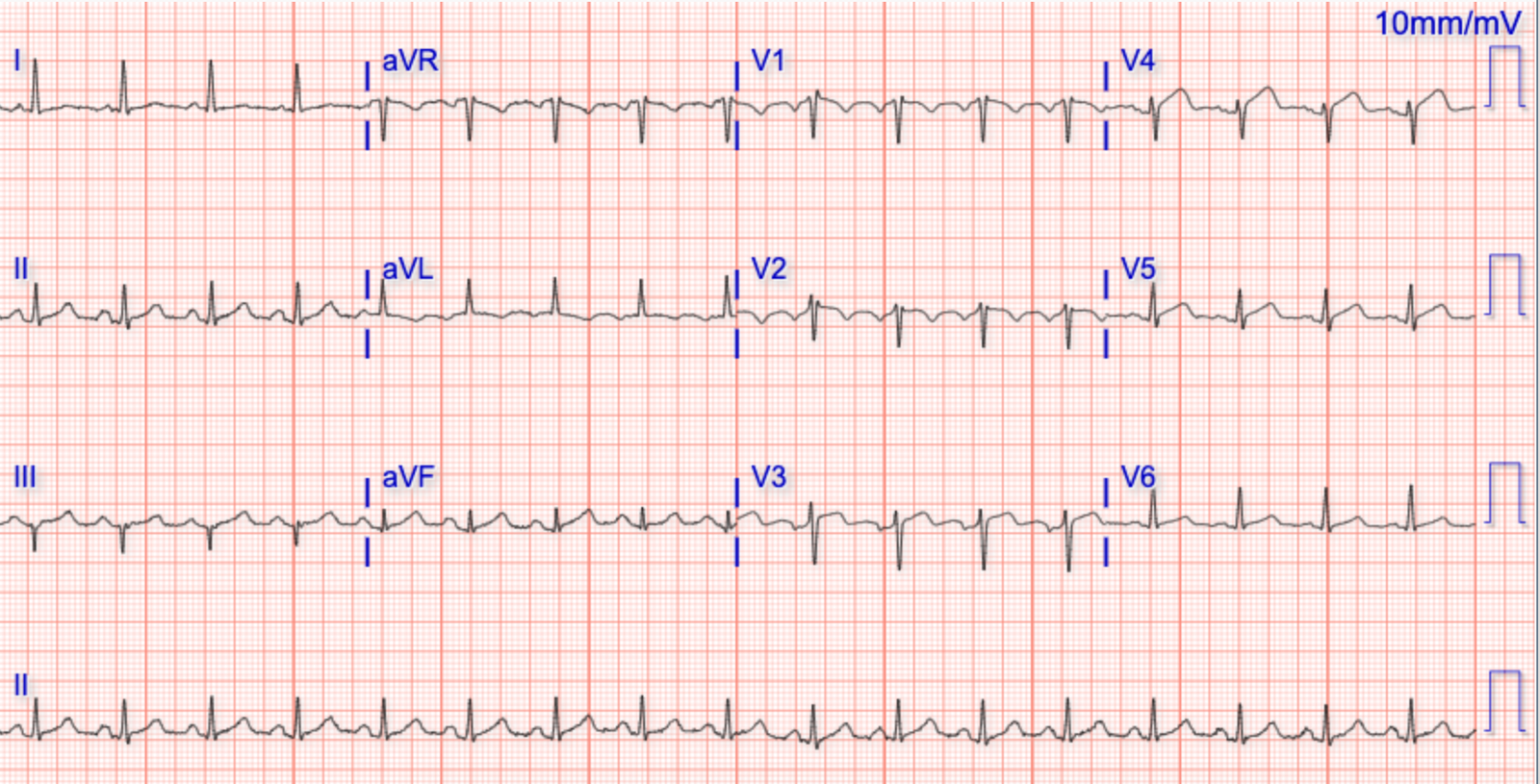
So they corrected the lead placement:
Here the leads are placed correctly:
 |
| Clearly a Posterolateral STEMI now.
The computer diagnosed it this time. |
This lead placement problem was not diagnosed by the medics. This resulted in a prolonged Door to Balloon Time. The resident did see it. The faculty did not, and learned a lot.
Angiogram:
Culprit was a 100% Occlusion of OM-1 (first obtuse marginal off the circumflex).
Learning Points
1. Young Women do have Acute MI. See here for more cases:
https://drsmithsecgblog.com/search/label/Young%20Women
2. Beware Lead placement! The computer will not always see it. STEMI can be missed. See Ken’s detailed comments below.
![]()
===================================
MY Comment by KEN GRAUER, MD (3/18/2020):
===================================
Recognition of technical errors is an often ignored, yet extremely important aspect of optimal ECG interpretation. That such technical errors remain prominent in everyday practice is immediately evident from random sampling of a series of tracings in any of the many international ECG internet forums. As a result — we like to periodically publish clinical examples of lead misplacement. To review a number of these — GO TO:
- The February 11, 2020 post.
- The November 4, 2018 post.
- The July 29, 2018 post.
There are many similarities between Today’s Case — and the February 11, 2020 post on Dr. Smith’s ECG Blog. Both patients presented with acute chest pain — which adds to the challenge of recognizing superimposed lead misplacement.
- By far — the most common lead reversal is mix-up of the LA (Left Arm) and RA (Right Arm) electrodes. This is the mix-up that occurred in both the Feb. post and in today’s case. Figure-1 (which I’ve adapted from the superb LITFL web page on this subject) — reviews the essentials of LA-RA reversal.

Figure-1: LA-RA Lead Reversal — adapted from LITFL (See text).
With the essentials from Figure-1 of LA-RA lead reversal in mind — Let’s TAKE ANOTHER LOOK at the initial ECG in this case (Figure-2):

Figure-2: The initial ECG in the ED — with features of LA-RA lead reversal written below the tracing (See text).
CHALLENGE — TRY TO ENVISION what this initial ECG (in Figure-2) would have looked like IF the limb leads were correctly placed.
ANSWER: In the bottom tracing of Figure-3 ( = ECG #1B, outlined in RED) — I have made the following changes:
- Lead I from ECG #1A has been inverted in ECG #1B.
- Leads II and III have switched positions.
- Leads aVL and aVR have switched positions.
- Lead aVF and the chest leads were left unchanged.
NOTE: As per Dr. Smith — correction of LA-RA lead reversal reveals acute postero-lateral OMI. This diagnosis is based on the following ECG features that we see in ECG #1B:
- Sinus rhythm (there now is an upright P wave in lead II of ECG #1B).
- Hyperacute ST-T waves in high-lateral leads I and aVL (as determined by T waves in these leads that are much fatter-at-their-peak and wider-at-their-base than expected).
- Reciprocal ST depression in each of the inferior leads — which is most marked in lead III, in which the shape of the depressed ST-T wave is a mirror-image opposite picture of the hyperacute ST-T wave in lead aVL.
- Anterior lead changes suggestive of acute posterior OMI — in the form of unexpectedly tall R waves in leads V2, V3 and a characteristic shape to the ST segment depression seen in leads V2 and V3, consistent with a positive Mirror Test (See My Comment in the February 16, 2019 post for illustration of the Mirror Test).
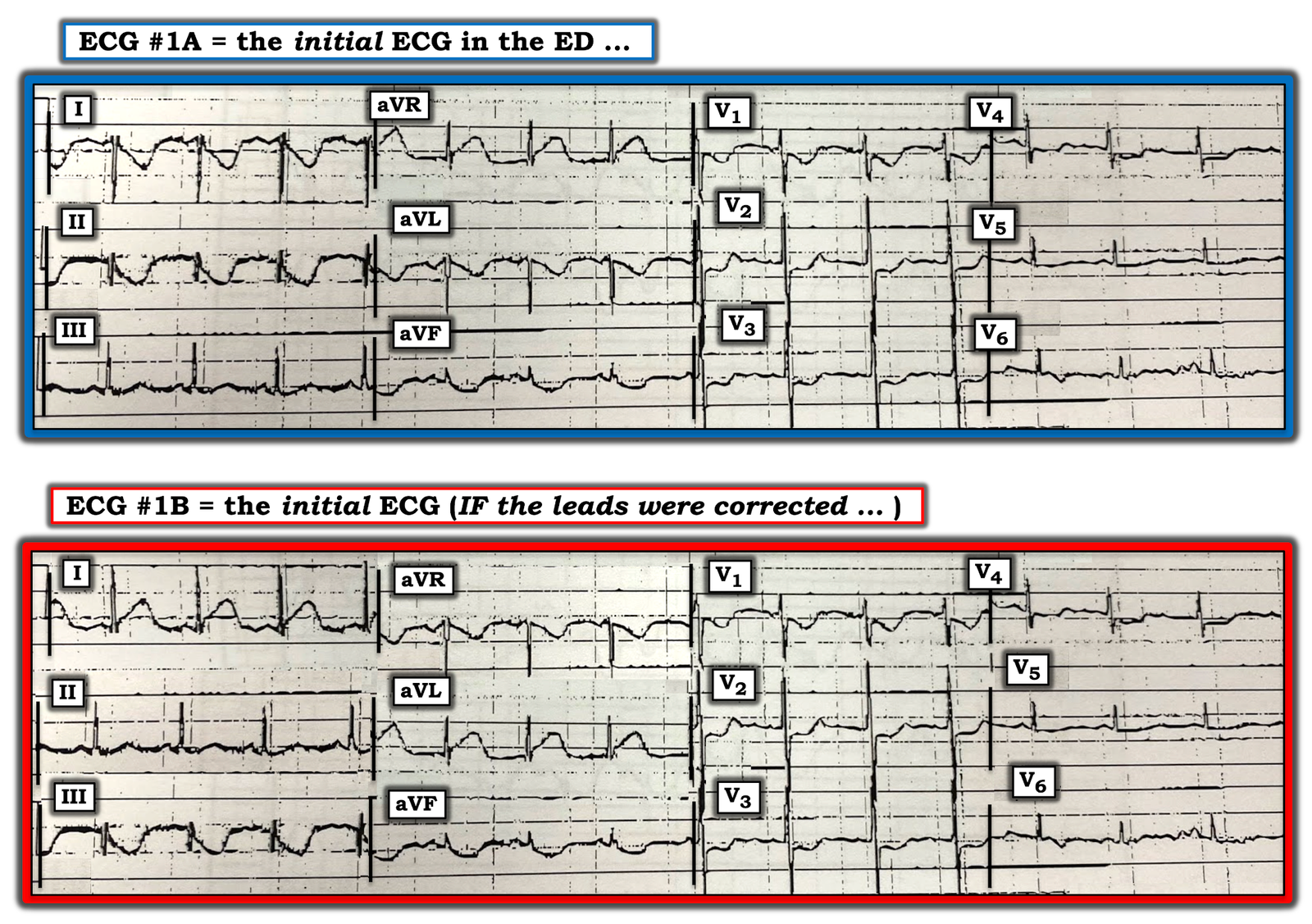
Figure-3: Comparison of the initial ECG in the ED ( = ECG #1A) — with what this ECG would look like IF: i) Lead I was inverted; ii) Leads II and III switched places; and, iii) Leads aVR and aVL switched places (See text).
KEY POINTS: As per Dr. Smith — This case is remarkable for lead misplacement in the initial ECG, that occurs in association with acute OMI. I’ll add the following points that have helped me to rapidly recognize this most common technical error of LA-RA lead reversal:
- You should never normally see global negativity (of the P wave, QRS complex and T wave) in lead I. If ever you do — then the diagnosis is either: i) Limb lead reversal; or, ii) Dextrocardia. Dextrocardia is rare (lead reversal is far more common!). With dextrocardia — there is reverse R wave progression (with much more rapid loss of R wave amplitude than what we see in ECG #1A).
- Lead aVR — most often manifests a predominantly negative QRS complex (often, but not always accompanied by a negative P and T wave). But the combination of a predominantly negative QRS in lead I with an upright QRS and upright T wave in lead aVR is distinctly unusual. IF lead I looks like you expect aVR to look — and, aVR looks like you expect lead I to look — then suspect LA-RA lead reversal!
- The P wave should be upright in lead II when there is sinus rhythm. IF you do not see an upright P wave in lead II — then you either have: i) a non-sinus rhythm; ii) some type of lead reversal; or, iii) dextrocardia. Note that NO P wave is seen in lead II of ECG #1A (although P waves are seen in leads I, III, aVL and aVF of this tracing). Then note that in ECG #1B — that an upright P wave now is seen in lead II, as expected with normal sinus rhythm.
- Finally — Please remember the easy-to-find superb web page on LITFL — that describes key findings in the 7 most common lead reversals: Simply put in, “LITFL Lead Reversal” into the Search bar — and this web page link will instantly come up!
![]()