

Written by Willy Frick
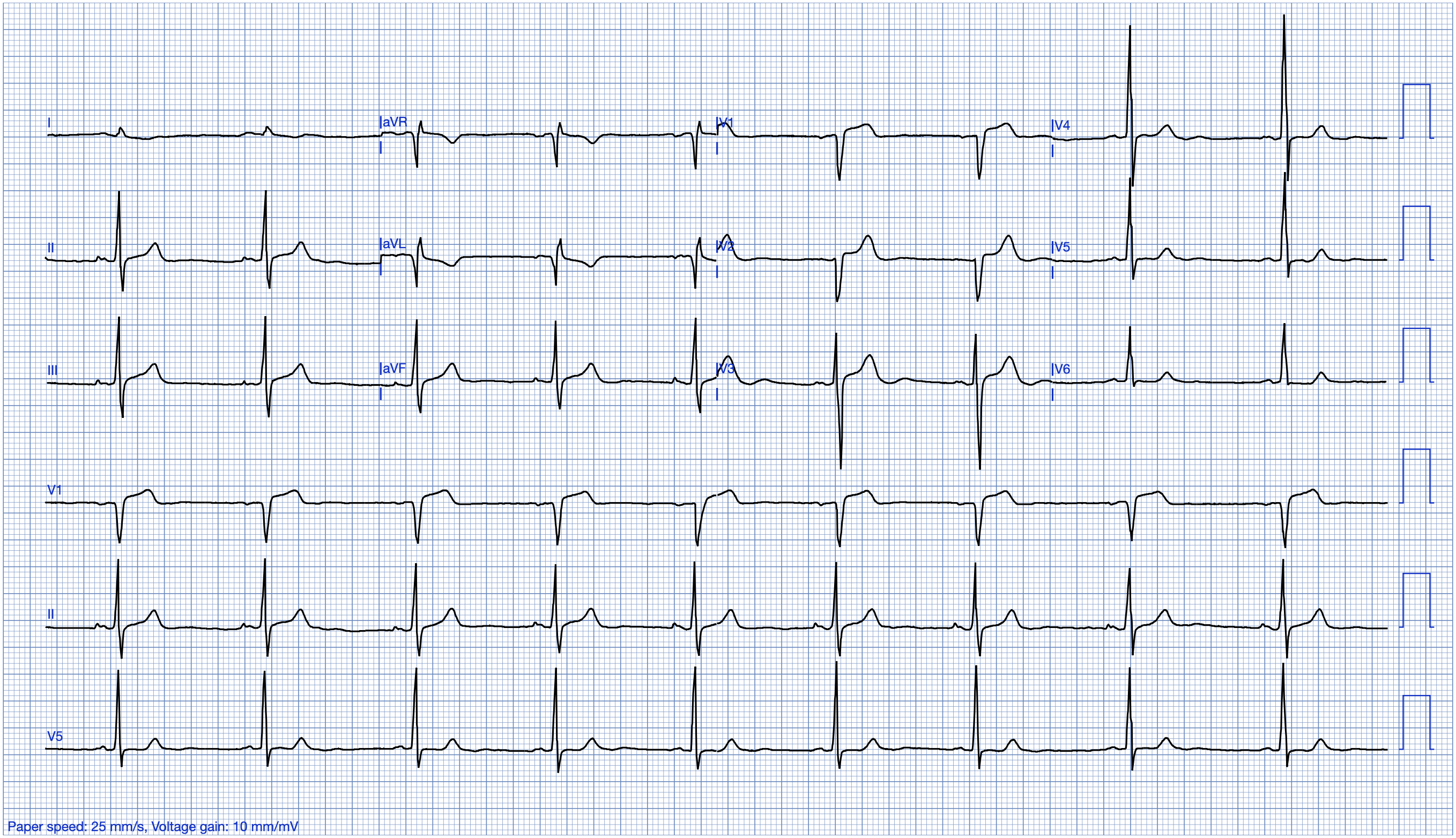
A man in his early 40s with no past medical history experienced acute onset crushing chest pain and dyspnea. The chest pain radiated into his left arm, and there was finger tip numbness. He rated it 10 out of 10. He took aspirin 325 mg and called EMS. The EMS report describes him as diaphoretic and clammy with extreme anxiety. His ECG is shown.
New PMcardio for Individuals App 3.0 now includes the latest Queen of Hearts model and AI explainability (blue heatmaps)! Download now for iOS or Android. (Dr. Smith is a shareholder in Powerful Medical.)


But it is easy to see why cases like this reinforce the biases of the physicians. Another NSTEMI where delaying cath did not appear to matter to the eventual outcome. That is how a STEMI disciple thinks of it. And in the world of STEMI, this is considered normal care. There is no way for this to be flagged as a systems failure for process improvement. Even though he had a large infarct (with classic symptoms), lost his septum, and experienced reduction in LVEF.
MY Comment, by KEN GRAUER, MD (6/14/2025):
- For clarity in Figure-1 — I’ve reproduced the 2 ECGs in today’s case.
- As we frequently emphasize — this clinical scenario immediately places this patient into a higher-risk likelihood for having an acute cardiac event (as it should be simultaneously lowering our “threshold” for activating the cath lab).
- The rhythm in ECG #1 is sinus bradycardia at a rate just under 60/minute — with normal intervals — a vertical frontal plane axis — and no chamber enlargement.
- My “eye” was immediately drawn to the 3 leads within the RED rectangles. Although subtle — there is straightening of the ST segment takeoff in lead V1, with a bit more than 1 mm of J-point ST elevation in this lead. Given very modest depth of the S wave in this V1 lead in this patient with crushing 10/10 new CP — this “picture” of the ST-T wave in lead V1 is definitely abnormal (and should be embedded in the brain of all emergency providers).
- Lead V2 “looks” funny (ergo the ? I added in Figure-1). That is — the J-point is elevated — then the ST segment itself is flat, followed by a disproportionately tall T wave considering modest depth of the S wave in this lead. Although a bit bizarre in appearance — the QRST complex in lead V2 supports our impression of an acute anterior event until proven otherwise.
- As emphasized in the numerous examples and my summary in the October 15, 2022 post — the entity of Precordial “Swirl” ( = acute proximal LAD occlusion) is recognized in a patient with new CP by abnormal ST elevation in leads V1,V2 — in a patient without LVH who manifests a flat (or scooped) and depressed ST segment in leads V5 and/or V6 (highlighted by the RED and BLUE arrows in these leads in Figure-1).
- There is no need to delay decision-making for Troponin levels (remembering that the initial 1-to-2 Troponins may be normal despite acute OMI).
- Given the history in today’s case and the above-described findings in ECG #1 — there is essentially nothing that might happen (ECG, Troponin or Echo-wise) to alter the need for prompt cath in this patient. So WHY wait?
- Other findings in ECG #1: With the exception of lead aVL — the limb leads in today’s initial tracing contribute little to our interpretation. Frankly — I did not know how to interpret the large Q wave and T wave inversion in lead aVL given lack of a similar appearance in the other high-lateral lead ( = lead I). Perhaps this T inversion in aVL reflects some component of reperfusion, possibly linked to the unusual appearance of the ST-T wave in lead V2?
-USE.png) |
| Figure-1: Side-by-side comparison of the initial EMS ECG — with the repeat ECG done ~1 hour later, when the patient’s CP returned. |
- KEY Point: Especially until definitive decision regarding whether to activate the cath lab is made — the ECG should be repeated whenever there is any change in the patient’s clinical condition. If impractical to repeat the ECG during transit (ie, with EMS rushing the patient to the hospital) — then as soon as the patient arrives in the ED — the ECG should be repeated. This apparently was not done.
- It was not until ~1 hour after the initial EMS ECG that return of this patient’s CP prompted the recording of a 2nd ECG ( = the repeat tracing shown in the bottom half of Figure-1).
- I thought lead-by-lead comparison of ECG #1 and ECG #2 showed essentially no change.
- The initial EMS ECG ( = ECG #1, recorded by EMS in the field when the patient was having 10/10 CP) — suggests Precordial “Swirl”, albeit ECG changes are somewhat subtle.
- Over the next 15 minutes — the patient’s CP decreased (albeit we do not know by how much his CP decreased — or if it resolved entirely). But no repeat ECG was done at this time.
- It was not until ~45 minutes later, when the patient’s CP “returned” — that a 2nd ECG was obtained. Comparison of this 2nd ECG with the initial EMS ECG did not show significant change.
- What would a repeat ECG obtained ~15 minutes after ECG #1 have shown, considering that CP had decreased at that time?
- If spontaneous reopening of the “culprit” artery was the reason this patient’s CP had decreased — we might have seen significant improvement in the ST-T wave abnormalities that were evident in ECG #1.
- And — IF spontaneous reclosure of the “culprit” artery was the reason for return of this patient’s CP ~45 minutes later — this might account for the ECG picture of ECG #2 that was obtained when CP returned.
MY Opinion: I completely agree with Dr. Frick that “improved” CP is not the same as “relieved” CP from an ischemic point of view (because as long as some CP is present in a patient with new ECG changes — there is ongoing ischemia that merits prompt cath with PCI to restore coronary flow).
- That said — since medical providers did not arrange for prompt cath after diagnostic ECG #1 was recorded — being able to demonstrate “dynamic” ST-T wave changes that correlate to a change in the relative severity of symptoms might have been possible IF a repeat ECG had been recorded ~15 minutes after ECG #1 when this patient’s CP had “decreased”.
- It is for this reason that I favor routine notation on the actual ECG of the presence and relative severity of CP as an extra insightful source for clinically determining the likely state of the “culprit” artery (ie, open or closed) — as well as for optimizing the chance of recording “dynamic“ ST-T wave changes that may serve to convince a reluctant interventionist of the need for prompt cath with PCI.


