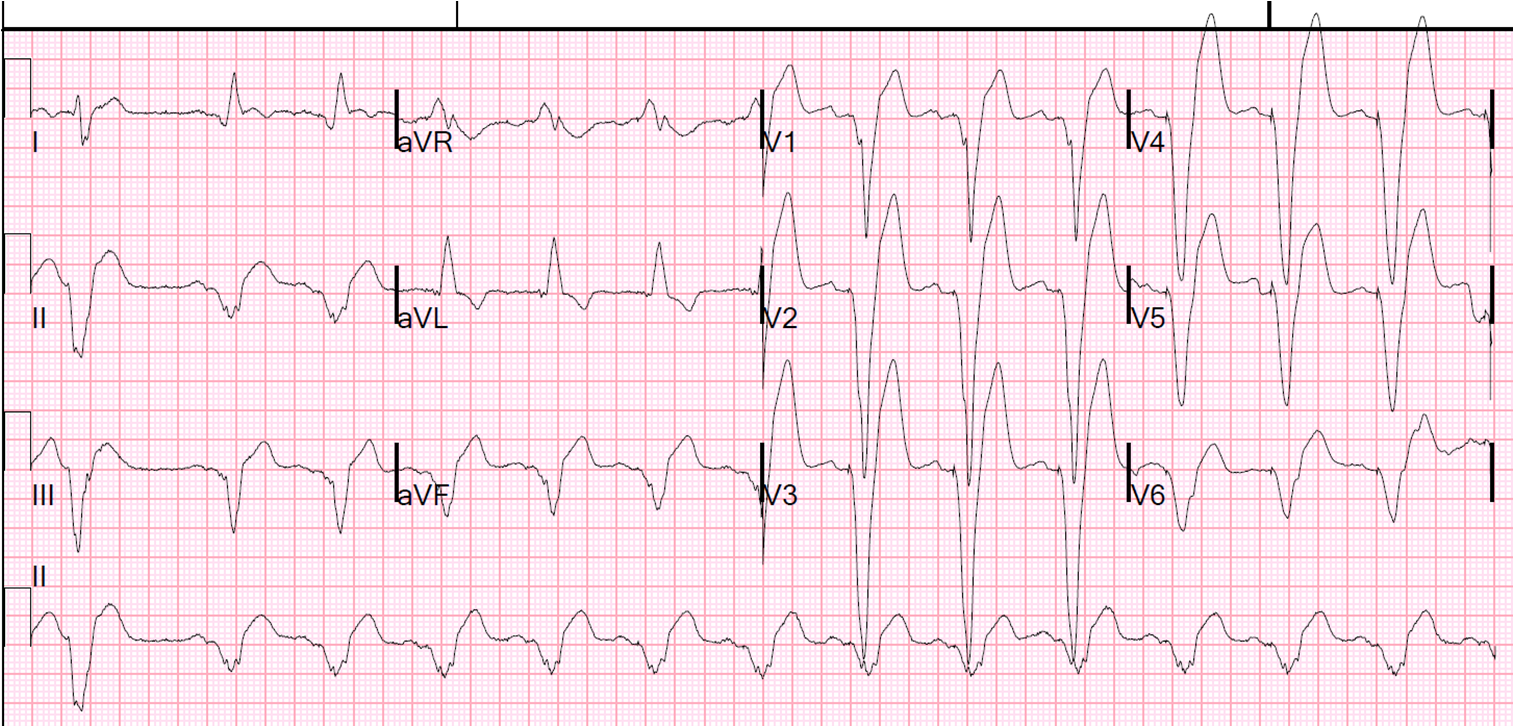
A middle age male presented with chest pain. Here is his ECG; there was no previous for comparison:
 |
| QTc is 380 ms. There is 3 mm of STE at the J-point in V2 and 2.5 mm in V3. There is also slight STE in aVL with reciprocal ST depression in III.
It is a rather scary ECG, very suggestive of proximal LAD occlusion (proximal would include the first diagonal, resulting in high lateral MI with STE in aVL and reciprocal ST depression in III). What is it? |
[There is also an upright T-wave in V1 and larger than the T-wave in V6 (some say this is a sign of STEMI – I have not found that it is a predictive independent variable)]
I immediately knew when I saw this that is was early repolarization. How?
First, what are the worrisome aspects?
1) what most catches the eye is the absence of an S-wave in V3. Normally, this is called “terminal QRS distortion” and is a very good sign of STEMI. However, it is NOT QRS distortion because, even though there is no S-wave, there is a very pronounced J-wave (a wave at the J-point).
2) The STE in aVL and STD in III suggest STEMI, but this is minimal ST deviation, and not enough to prevent use of the LAD occlusion vs. early repol formula (see sidebar excel applet).
With QTc 380
STE at 60 ms after the J-point in V3 = 2.5
R-wave amplitude in V4 = 28
Result = 16.3, which is far less than the cutoff of 23.4
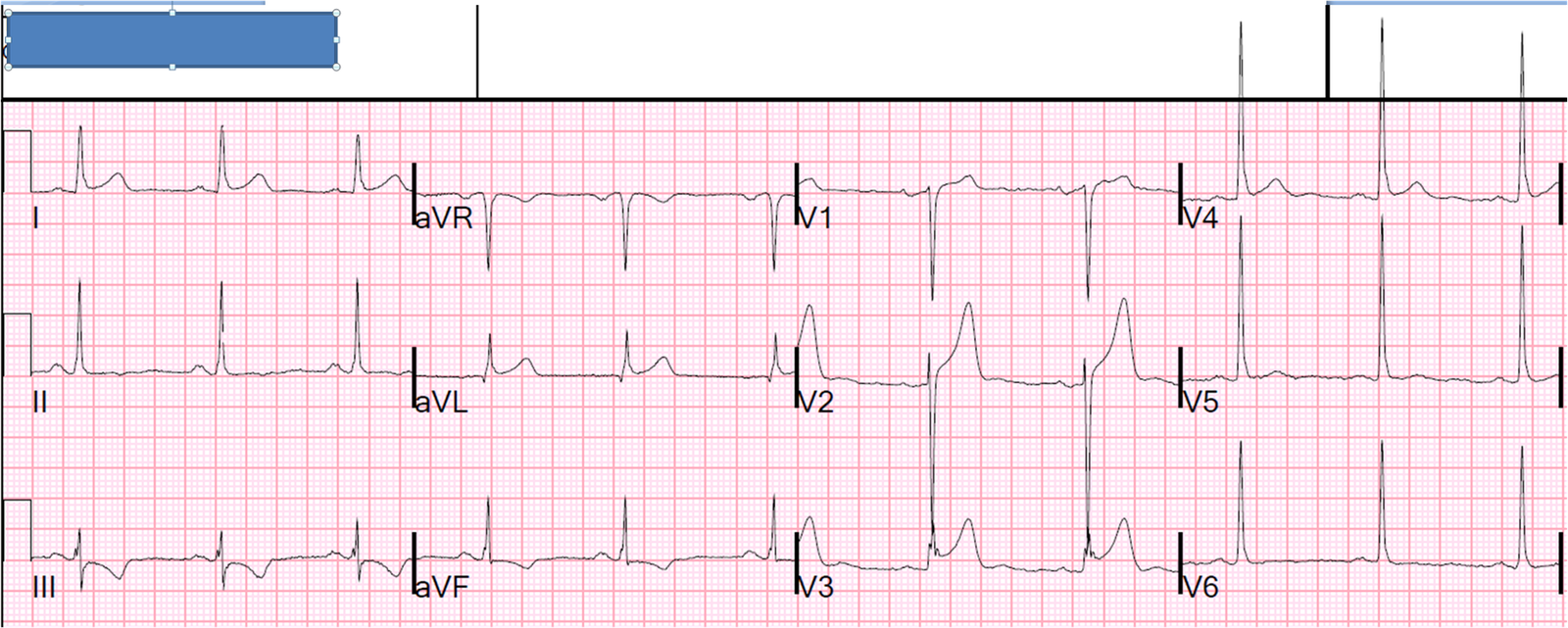
We did serial ECGs and there was no change. He ruled out for MI with serial troponins. (Ruling out alone is not proof, however — This is a GREAT CASE)
The reciprocal relationship between aVL and III should still be bothering some. Below is an explanation that is further elaborated upon in this post:
Here is a post on True positive vs. false positive ST elevation in aVL, with illustrative cases
When there is ST elevation in aVL, with reciprocal ST depression in III:
1. Look for these signs of MI:
a. Absence of J-waves
b. Other ST depression
c. Large T-waves
d. Symmetric T-waves
e. Down-Up T-waves
2. Compare with an old ECG
3. Use ED Echo if available
4. Use formal Echo
5. A positive troponin is helpful (a negative one is not if symptoms are of few hours duration or less)