Written by Magnus Nossen
A woman in her thirties contacted the ambulance service because of progressive shortness of breath. She reported being pregnant and had initially attributed her symptoms to the pregnancy. A few days earlier she had visited her primary care physician, where a 12‑lead ECG was obtained. As her dyspnea had worsened rapidly over the preceding couple of days, she decided to seek emergency medical assistance.
Below is the 12‑lead ECG recorded three days earlier in her general practitioner’s office. This ECG was described as normal. What do you think?
ECG #1
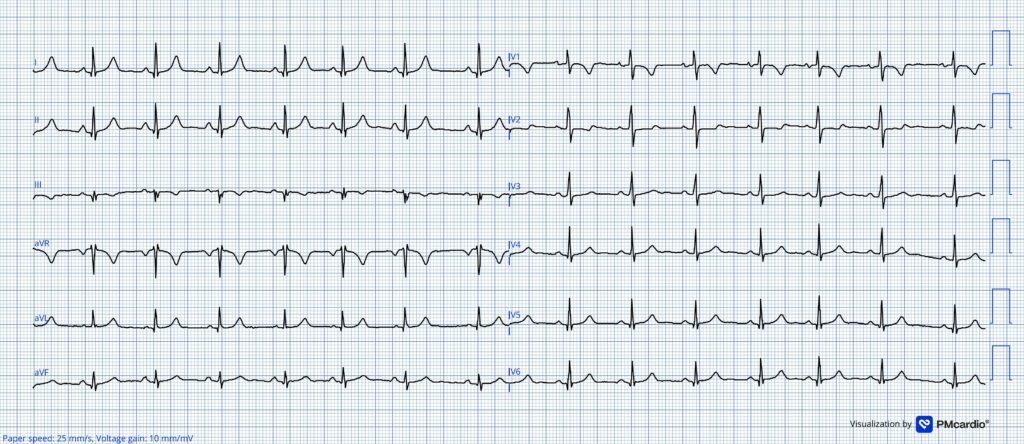
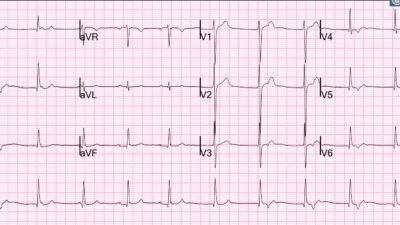
This ECG shows sinus rhythm at 80 beats per minute. There are T wave inversions present in lead V1 and III. The is R>S in lead V1, which is abnormal. The QRS axis is 5 degrees and the T wave axis is 23 degrees. This gives a low QRST angle meaning the TWI in lead III could be a normal variant. (For an in-depth discussion on T wave inversions and QRST angle have a look at this lecture by Dr. Smith. Also see Dr. Grauer comment below for more on R/S ratio in V1.)
Apparently, the clinic physician sent the patient home.
Smith: Although there is no right axis deviation, the large R-wave in V1 strongly suggests RVH. The patient should get an echocardiogram. In any case, a patient with dyspnea should never be sent home unless there is a definite diagnosis, and that diagnosis is not a dangerous one.
Now back to the present day when she called the ambulance: When EMS arrived, they found a visibly ill patient who was tachypneic and tachycardic, with an oxygen saturation in the low 90s and a heart rate of approximately 125 beats per minute. The patient appeared anxious, complaining of breathlessness — but denied chest pain. She was given oxygen and transported to the nearby emergency department only a few minutes away.
Upon arrival in the emergency department, the patient had a brief episode of altered mental status followed by syncope. After this syncopal episode, she remained profoundly hypotensive and in severe distress. An ECG was obtained immediately and is shown below. Based on the clinical presentation and the ECGs provided in today’s case, what is the most likely diagnosis?
ECG #2
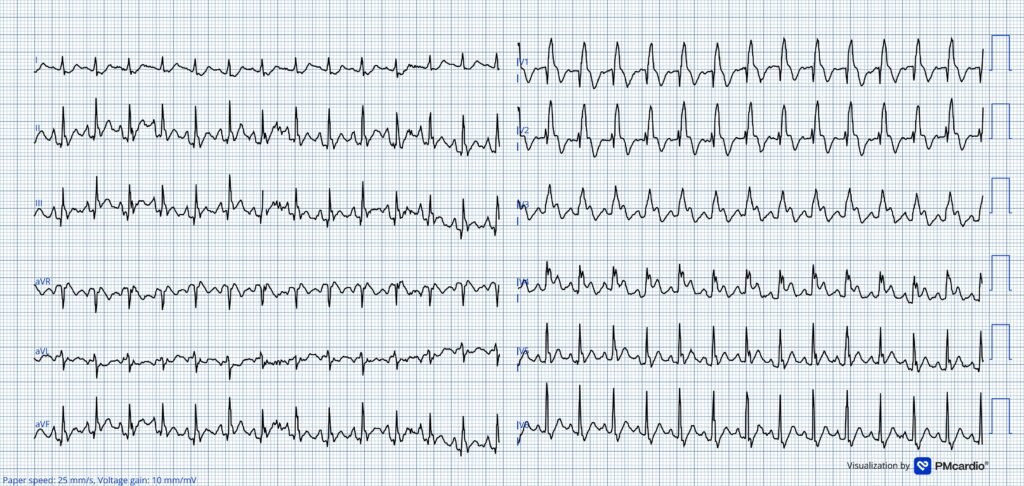
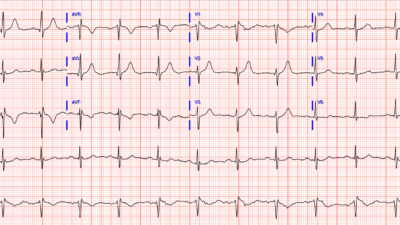
This ECG shows sinus tachycardia at 156 bpm. Compared to the previous ECG from three days ago — there is a new RBBB with concordant ST-elevation and TWI in leads V1-V3, and concordant ST elevation with concordant T wave in lead V4.
Sinus tachycardia is rare in OMI unless there is new cardiogenic shock. It is of course possible that the ECG changes could be due to OMI — and pregnancy does increase the risk of spontaneous coronary artry dissection (SCAD). However, the clinical picture in today’s case is not typical of OMI — as there is acute superimposed on subacute dyspnea and no chest pain.
Smith: ACS or OMI only causes hypoxia if it causes pulmonary edema. (slight exception: If there is shock, then poor peripheral perfusion may give an artifactually low pulse oximeter reading, but not actual low arterial pO2). This is a case in which the diagnosis a clinial diagnosis, NOT an ECG diagnosis. The ECG is compatible with the diagnosis of PE.
A more plausible explanation is obstructive shock due to a massive pulmonary embolism. This diagnosis was immediately made on clinical grounds, strongly supported by point-of-care ultrasound demonstrating a severely dilated right ventricle and underfilled LV ( = findings consistent with acute right ventricular pressure overload). Systemic thrombolytics were administered emergently, and the patient was intubated for airway protection and respiratory failure.
Smith: beware of intubation in pulmonary embolism patients in shock. Emergency intubation in any RV failure patient (acute or chronic) may be necessary but is very has a high risk of hemodynamic collapse. This study was recently published: Characteristics and Short-Term Outcomes of Patients With Acute Pulmonary Embolism Requiring Intubation. Acad Emerg Med. 2026 May;33(5):e70317. doi: 10.1111/acem.70317. PMID: 42084455.
Case continued: Following thrombolysis, her hemodynamic status improved rapidly, and once stabilized — CT pulmonary angiography confirmed the diagnosis of acute pulmonary embolism.
In the context of sudden, massive pulmonary embolism causing obstructive shock — the ECG may show ST-elevation in right-sided precordial leads. These changes can be explained by transmural right ventricular ischemia from severely reduced right ventricular coronary perfusion.
Smith: the ECG findings can mimic those of RV infarction, with STE in V1-V3.
In the normal state, the right ventricle is perfused continuously throughout the cardiac cycle because its systolic pressure remains below the systemic diastolic pressure. This allows uninterrupted flow in the right coronary artery. In the setting of a massive pulmonary embolism, pulmonary vascular resistance can rise abruptly. This acutely increases right ventricular systolic pressure. At the same time — left ventricular stroke volume and cardiac output fall due to obstructive shock, lowering coronary perfusion pressure. The above combination of events may critically reduce right coronary artery flow and lead to transmural right ventricular ischemia. The end result of these hemodynamic changes may precipitate syncope, shock and/or cardiac arrest.
Given that the Queen of Hearts AI is trained to detect patterns consistent with occlusion myocardial infarction — it is not perhaps then surprising that the AI model interpreted ECG# 2 as STEMI equivalent (albeit with low confidence).
= = =
= = =
Back to the Case:
As noted, the patient’s hemodynamics improved rapidly after thrombolysis. An ECG was obtained 10 hours later, by which time her heart rate had fallen below 100 beats per minute.
ECG #3

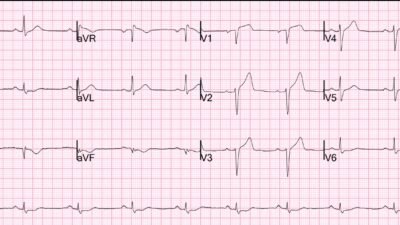
The ST-elevation is now gone and the heart rate has dropped significantly. There is still RBBB. TWI extending though V1-V4. There is also a Q wave and TWI in lead III (Q3T3).
Discussion:
The initial ECG in this case shows TWI in lead III and V1. The QRST angle was low which might be reassuring — however morphology and depth of the T‑wave inversion in lead V1 (as seen in ECG #1) is worrisome. T‑wave inversion in lead III occurs in about 2–10% of asymptomatic adults and can be a normal variant. However, if the patient presents with new dyspnea onset dyspnea and the ECG shows TWI in lead III — the possibility of an acute PE event should be considered even if the QRST angle is normal. This patient did not present with a clinical picture consistent with ischemia.
Kosuge and colleagues demonstrated that simultaneous T‑wave inversion in leads V1 and III (the Kosuge sign) helps discriminate between acute coronary syndrome or pulmonary embolism: this pattern was present in 88% of patients with pulmonary embolism, but in only 1% of those with acute coronary syndrome.
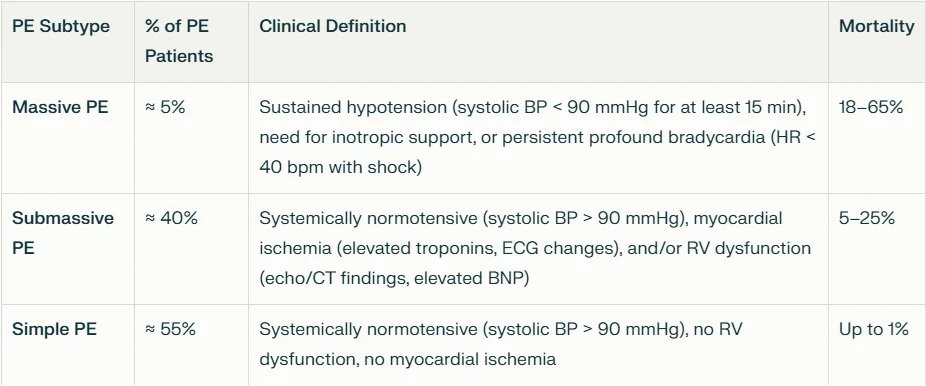
Our patient likely experienced multiple pulmonary emboli, leading to progressively worsening dyspnea and ultimately hemodynamic collapse. Pulmonary embolism is commonly categorized as massive, submassive, or low‑risk (simple), and their respective characteristics and mortality rates are summarized in table 1 below.
Table 1
= = =
Want to become better at recognizing acute PE?
Have a look at the below cases for more examples of pulmonary embolism and associated ECG findings.
- Anterior T wave inversion due to Pulmonary Embolism – Dr. Smith’s ECG Blog
- Is this ECG easy for you yet? – Dr. Smith’s ECG Blog
- ECG interpretation can keep you out of the courtroom. And “viral infection” by itself is not an explanation for dyspnea – Dr. Smith’s ECG Blog
- Can you guess the diagnosis? – Dr. Smith’s ECG Blog
- A woman in her 40s with acute chest pain and shortness of breath – Dr. Smith’s ECG Blog
- A man in his 50s with shortness of breath
- Another deadly triage ECG missed, and the waiting patient leaves before being seen. What is this nearly pathognomonic ECG?
- A man in his 40s with RUQ abdominal pain
- A woman in her 50s with shortness of breath
- When the ECG is more revealing than the HPI
- A crashing patient with an abnormal ECG that you must recognize
- A man in his 40s with a highly specific ECG
- Chest pain, ST Elevation, and tachycardia in a 40-something woman
- Repost: Syncope, Shock, AV block, RBBB, Large RV, “Anterior” ST Elevation in V1-V3
- A young woman with altered mental status and hypotension
- An elderly woman transferred to you for chest pain, shortness of breath, and positive troponin – does she need the cath lab now?
- A 30-something woman with chest pain and h/o pulmonary hypertension due to chronic pulmonary emboli
- A 30-something with 8 hours of chest pain and an elevated troponin
- Syncope, Shock, AV block, Large RV, “Anterior” ST Elevation….
- Dyspnea, Chest pain, Tachypneic, Ill appearing: Bedside Cardiac Echo gives the Diagnosis
- 31 Year Old Male with RUQ Pain and a History of Pericarditis. Submitted by a Med Student, with Great Commentary on Bias!
- Chest pain, SOB, Precordial T-wave inversions, and positive troponin. What is the Diagnosis?
- Cardiac Ultrasound may be a surprisingly easy way to help make the diagnosis
- Answer: pulmonary embolism. Now another, with ultrasound….
- This is a quiz. The ECG is nearly pathognomonic. Answer at bottom.
- Chest Pain, SOB, anterior T-wave inversion, positive troponin
- Anterior T wave inversion due to Pulmonary Embolism
- Collapse, pulse present, ECG shows inferior OMI. Then there is loss of pulses with continued narrow complex on the monitor (“PEA arrest”)
- What do you suspect from this ECG in this 40-something with SOB and Chest pain?
= = =
Learning Points:
- TWI in lead III may be normal, but in the setting of acute dyspnea, PE must be considered as a possible explanation. This is especially true in the context of other suggestive findings such as tachycardia, hypoxia or risk factor for thromboembolism.
- If there is massive PE with hemodynamic compromise — thrombolytics are often life saving.
- The RV normally receives blood supply throughout the cardiac cycle. Acute PE may disturb RV coronary perfusion — thereby resulting in RV transmural ischemia.
- The RV is compliant and tends to dilate in response to acute afterload increase. This may impair left ventricular filling and cardiac output —further worsening hemodynamics.
= = =
==================================
MY Comment, by KEN GRAUER, MD (6/5/2026):
Whereas some shortness of breath is most often a common physiologic accompaniment of a normal pregnancy — progressive dyspnea severe enough to prompt a visit to the patient’s physician (as occurred in today’s case) — is cause for concern that there may a serious problem. Among the lessons conveyed by today’s case are:
- i) Be on the alert for subtle signs of ECG abnormalities; — and —
- ii) Have a low threshold for doing an Echo in pregnant patients with progressive dyspnea (Echo being an excellent noninvasive test for picking up peripartum cardiomypathy and pulmonary emboli = the 2 major potentially life-threatening causes of progressive dyspnea in pregnancy that may at first be deceptively subtle).
= = =
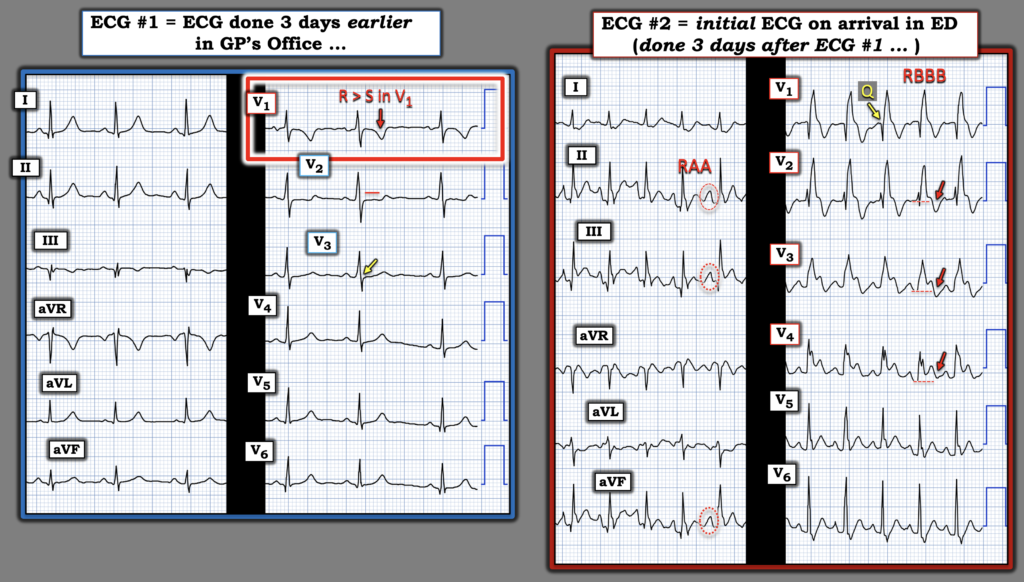
ECG #1: Done 3 days earlier in the GP’s Office …
For clarity and ease of comparison in Figure-1 — I’ve put the 1st ECG done in today’s case (recorded by the patient’s primary care physician) together with the initial ECG done 3 days later on arrival to the ED. Prior to reading what happened in this case — I interpreted this 1st ECG (done 3 days before the initial ED ECG) as non-diagnostic, but abnormal and clearly suspicious of a right-sided problem.
- Although an R wave greater than the S wave in lead V1 is common in childhood (being the rule rather than the exception up to 5 years of age) — a Tall R Wave in Lead V1 (ie, an R>S in V1) — is usually not a normal finding in adults. In a pregnant woman with dyspnea — this finding should prompt consideration of RVH.
- NOTE: Physiologic adaptations in normal pregnancy have been associated with ECG changes, including a slight left-sided shift in frontal plane axis (attributed to a rising diaphragm as pregnancy advances) — and on occasion, T wave inversion in leads III; and/or leads V1,V2,V3 (Ananthakrishnan et al — J Mar Med Soc 22:187-192, 2020). That said — these changes should not be expected to alter the normal predominant S>R wave ratio in lead V1.
- In support of my suspicion that the R>S ratio in V1 may indeed be an abnormal finding were the following: i) I interpreted the surprisingly deep, symmetric T wave in lead V1 as disproportionately large given modest overall QRS amplitude in this lead; — ii) The ST-T wave in lead V2 is flat and appears to be slightly depressed — whereas the ST-T wave in leads V2,V3 normally display gentle upsloping and slight ST elevation; — iii) Although the ST segment in lead V3 is upsloping — there is no J-point elevation (YELLOW arrow in this lead) — and, iv) There is clear T wave inversion in lead III (and in view of the tiny s wave in lead I — an S1Q3T3 pattern is suggested).
- My Conclusion: Although possible that the above described ST-T wave changes in leads III; V1,V2,V3 were all part of a physiologic adaptation to pregnancy (as per the above cited Ananthakrishnan article) — in association with the abnormal R>S ratio in lead V1, these findings could represent a subtle developing pattern of RV “strain”.
- Therefore — In a pregnant patient with progressive dyspnea and an ECG with subtle signs of potentially attributed to RV “strain” — an Echocardiogram could serve as a quick, noninvasive test to either reassure or confirm right ventricular abnormalities in need of prompt evaluation.
= = =
Figure-1: Comparison of the 1st ECG (done 3 days earlier in the office of the patient’s GP) — with ECG #2, done on arrival in the ED.
= = =
ECG #2: The Initial ECG done on arrival in the ED …
By the time ECG #2 was recorded — the patient’s condition had dramatically worsened. As per Dr. Nossen — this initial ED tracing showed the alarming findings of:
- Marked sinus tachycardia (over 150/minute).
- Complete RBBB (Right Bundle Branch Block).
- ST elevation in leads V1-thru-V4. I found it interesting that in leads V2 and V3 (and to a lesser extent in lead V4) — despite marked ST elevation, there was surprisingly deep terminal T wave inversion in these leads (RED arrows in leads V2,V3,V4).
- ST “elevation” actually begins in lead V1 — since normally with RBBB there should be ST depression in lead V1, whereas the J-point in this lead is isoelectric.
- PEARL: On occasion, anterior ST elevation (instead of T wave inversion) can be seen as a sign of acute PE (Zhan et al — Ann Noninvasive Electrocardiol 19(6):543-551, 2014 – and – Omar HR — Eur Heart J: Acute Cardiovasc Care 5(8):579-586, 2016). I therefore interpreted the fact that despite the marked ST elevation that we see in leads V1-thru-V4 — there is still deep anterior T wave inversion as indication of severe RV “strain” in ECG #2.
Two additional findings of interest consistent with the severity of this patient’s massive acute PE were:
- i) RAA (Right Atrial Abnormality) — as indicated by the tall, peaked and pointed P waves ≥2.5 mm in one or more of the inferior leads. (NOTE: RAA was not present in ECG #1!).
- ii) Instead of the typical rSR’ pattern of RBBB — there is a QR pattern in lead V1. In the setting of RBBB, the loss of the initial positive r wave deflection, to form a qR pattern in Lead V1 suggests there is pulmonary hypertension! (See my Figure-2 in My Comment at the bottom of the page in the February 12, 2023 post for illustrated discussion of why this is so).
= = =
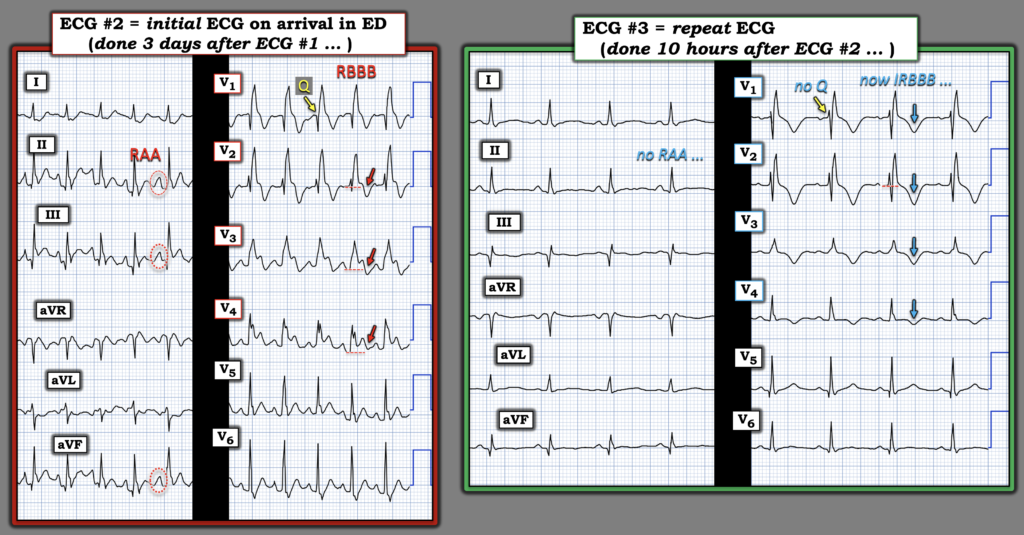
Figure-2: Comparison of ECG #2 — with the repeat ECG done 10 hours later, after clinical improvement.
= = =
ECG #3: The Repeat ECG done 10 hours after ECG #2 …
I found it of interest in the comparison of ECG #2 and ECG #3 (as shown above in Figure-2) — to see significant improvement in the ECG findings of acute RV “strain” corresponding to the marked clinical improvement in this patient’s condition after 10 hours of treatment.
- As per Dr. Nossen — the patient’s heart rate has returned in ECG #3 to a normal rate range.
- The QRS has narrowed from ≥0.12 second when RBBB was “complete”, as it was in ECG #2 — to ~0.10-0.11 second in ECG #3 (with significant narrowing of the terminal S wave in left-sided lead V6) — now being more consistent with an incomplete RBBB pattern.
- The Q wave in lead V1 that was seen in ECG #2 — is no longer present in ECG #3 (suggesting there most probably has been improvement in the Echo findings of severe RV dilation, with corresponding reduction in pulmonary pressure).
- ECG criteria for RAA are no longer present in ECG #3.
- Finally — the anterior ST elevation that was so prominent in ECG #2 — has virtually resolved (which probably accounts for why the anterior T wave inversion in ECG #3 now seems so much more evident despite all clinical indicators suggesting reduced RV “strain”).
The “good news” in today’s case — is that prompt recognition in the ED of fulminant obstructive shock from massive acute PE, resulted in immediate initiation of life-saving thrombolytic therapy.
= = =
= = =