From Avery Kechter in Cork, Ireland (Avery is a former resident at Hennepin who married another former resident who is Irish. They recently moved to Ireland and are both working EM there!)
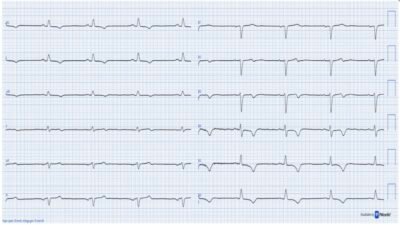
A 30-something man presented with waxing and waning chest pain. This ECG was recorded:
What do you think?
Smith: I think this is equivocal. The T-waves in inferior leads and in V4-6 are large with some hyperacute features, but they also have a lot of upward concavity, such that they do not look very inflated. However, there is reciprocal T-wave inversion in aVL (with perhaps a hint of STD) and the same in V2, but very suggestive of inferior-posterior OMI (along with lateral in V4-6). I don’t think it is diagnostic, but I would activate the cath lab and take a look at the coronary arteries.
Here is the PMCardio Queen of Hearts AI Model, with heat map explainability:

The Queen sees many of the features that I mentioned, and gives an output of 0.99, which is very certain of OMI.
New PMcardio for Individuals App 3.0 now includes the latest Queen of Hearts model and AI explainability (blue heatmaps)! Available in the EU — Download now for iOS or Android. https://www.powerfulmedical.com/pmcardio-individuals/ Hopefully will get FDA approval soon for American users. (Drs. Smith and Meyers trained the AI Model and are shareholders in Powerful Medical). As a member of our community, you can use the code DRSMITH20 to get an exclusive 20% off your first year of the annual subscription. Disclaimer: Certain AI ECG Modules are CE-marked medical devices under EU MDR and are certified for marketing only in the European Union and the United Kingdom. PMcardio technology has not yet been cleared by the US Food and Drug Administration (FDA) for clinical use in the USA.
Clinical Course
The conventional computer algorithm gave a diagnosis of “Normal ECG“. It was shown to the triage physician who signed off as “Normal/No concern.”
Avery did not see the ECG until the first hs troponin I returned at 3500 ng/L. And the ECG alarmed him.
He rapidly activated the cath lab despite quite a bit of “skepticism from cardiology.”
Angiogram: showed clean coronaries
Echocardiogram: no WMA, Peak troponin I was 6800 ng/L
Cardiac MR confirmed myocarditis
Learning point:
- This could easily have been OMI but the findings were missed by the doctor who first read the ECG. Use of the Queen of Hearts can avoid such oversights. (See below our study from JACC: Cardiovascular Interventions)
- The conventional algorithms frequently will mark as completely normal an ECG that manifests OMI !! We showed this in this study: Artificial Intelligence Detection of Occlusive Myocardial Infarction from Electrocardiograms Interpreted as “Normal” by Conventional Algorithms
- Myocarditis can very extremely difficult to differentiate from OMI. The ECG can exactly mimic OMI.
- a. There is usually a wall motion abnormality in the location that correlates with the ECG.
- b. Even an angiogram alone cannot tell you whether the outcome is MINOCA (Myocardial Infarction with Non-Obstructed Coronary Arteries) or myocarditis.
- c. Other data such as CRP, presence of viral illness, etc are non-specific.
- d. Presence of a friction rub or pericardial effusion may be helpful for myo-pericarditis.
- Really, in order to rule out OMI, you need either
- 1) intracoronary imaging [Optical Coherence Tomography (OCT) or Intravascular Ultrasound (IVUS)] or
- 2) Cardiac MRI.
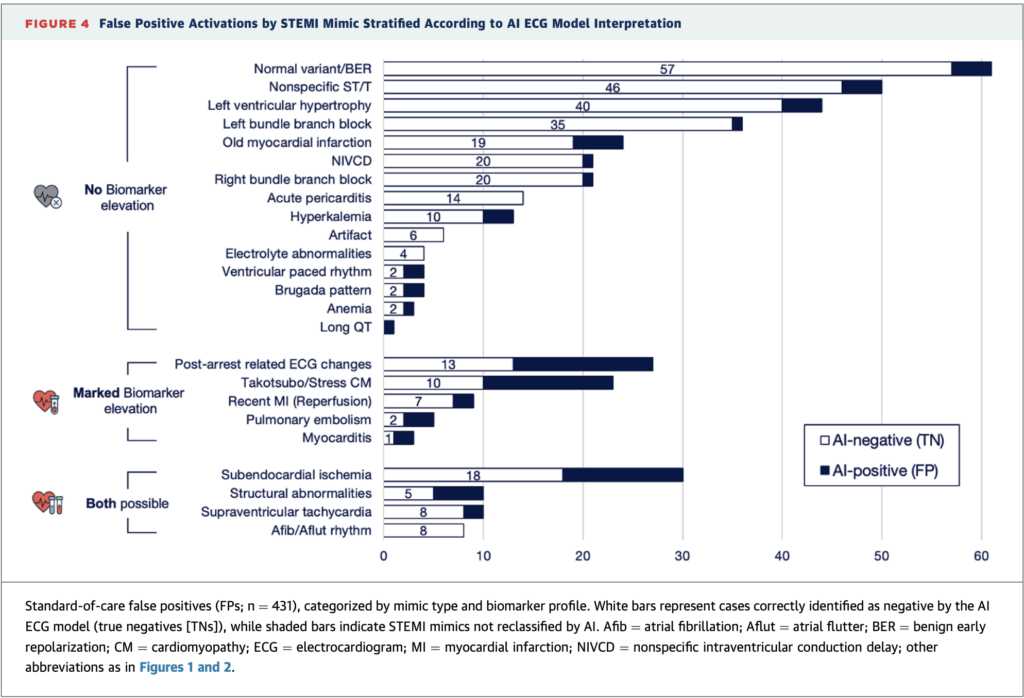
See this study: AI-Enabled ECG Analysis Improves Diagnostic Accuracy and Reduces False STEMI Activations: A Multicenter U.S. Registry. We showed that the Queen of Hearts decreases false positive cath lab activations from 42% to 8%. HOWEVER, in cases with elevated troponins such as myocarditis and takotsubo, it was much more difficult to differentiate a mimic from OMI.
= = =
======================================
MY Comment, by KEN GRAUER, MD (4/17/2026):
It’s cases like the one presented today that always remind me of my general surgery rotation — in which we were told that the surgeon who was 100% accurate in predicting which patients had acute appendicitis was not operating on enough patients. The point of this truism is that we need to accept we will not predict with 100% accuracy which patients with CP (Chest Pain) need prompt cath. As a result — a normal cath does not necessarily mean that cath lab activation was wrong, but rather that cath lab activation is appropriate to rule out an acute OMI in suspicious cases — even when the catheterization turns out to be normal (as it did in today’s case).
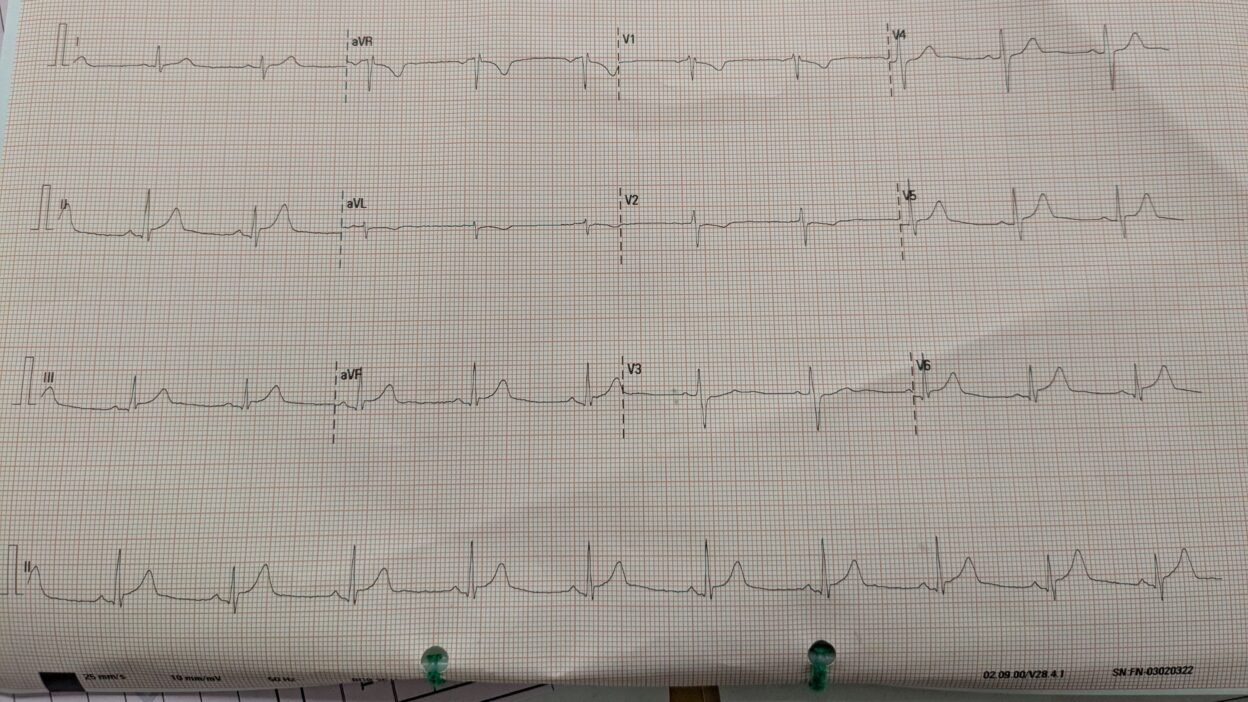
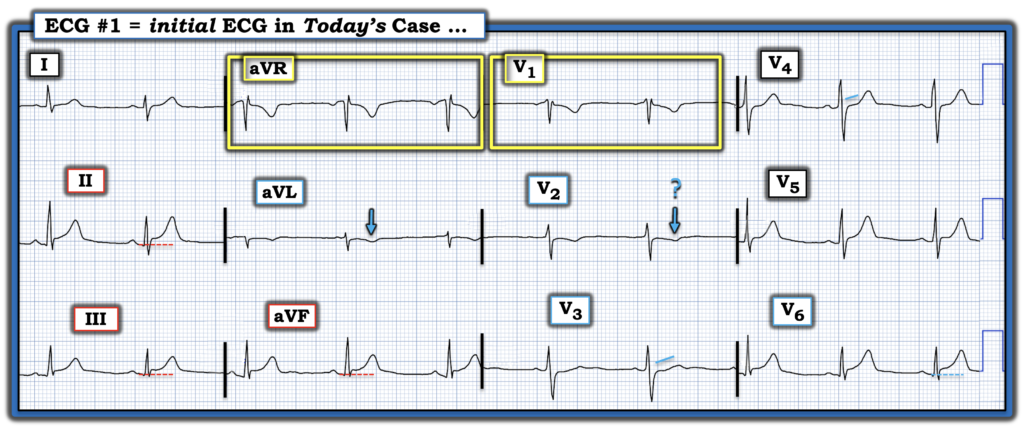
- For clarity in Figure-1 — I’ve labeled today’s initial ECG.
- I interpreted this ECG before looking at the Answer. My interpretation was similar to that of Dr. Smith, namely that this tracing is non-diagnostic — but with a number of features suggestive enough of acute infero-postero-lateral OMI that prompt cardiac cath is indicated!
= = =
The ECG in Figure-1:
The rhythm in today’s initial ECG is sinus with normal intervals, axis and no chamber enlargement. R wave progression is normal — and other than the tiny septal q wave in lead V6, there are no Q waves.
- Given the history of “waxing and waning CP” — my “eye” was immediately drawn to the ST elevation with prominent T waves in leads II,III,aVF.
- As per Dr. Smith — the upward concavity ( = “smiley” configuration) shape of ST segments in these 3 inferior leads is a point against an acute event — but the inescapable finding of potential reciprocal change in lead aVL (in the form ST segment flattening with slight depression and a bigger-than-it-should-be inverted T wave) in a patient with new CP suggests acute OMI until proven otherwise.
- Unfortunately — assessment of lead V1 in Figure-1 is invalidated by too high electrode lead placement. This is relevant to today’s case — because confirmation of inferior OMI is often forthcoming from ECG evidence of posterior OMI, which is rendered more difficult when the validity of leads V1,V2 is in question. As shown within the YELLOW rectangles in Figure-1 — lead V1 misplacement is suggested by the rSr’ pattern with negative P wave and QRST morphology that closely resembles lead aVR. (See our Technical Misadventures Tab at the top of every page in this ECG Blog for multiple examples of V1-V2 misplacement).
- I found lead V2 difficult to assess because some of the T wave inversion might be related to lead V2 misplacement (so common when the V1 electrode is misplaced) — but ST segment straightening and loss of the upsloping, slightly elevated ST segment that is normally seen in lead V3 suggests associated posterior OMI.
- Finally — ST segment elevation in lead V6, with an overall ST-T wave shape similar to that seen in the inferior leads suggests lateral involvement.
- Bottom Line: The ECG in Figure-1 is not “normal”, and not “of no concern” (as described by the triage physician who signed off of today’s case). Instead — in a patient with new CP — although non-diagnostic, I thought today’s initial ECG suspicious enough to merit prompt cath.
- The significantly elevated Troponin confirmed the need for this procedure.
- Learning Point: Acute myocarditis may at times produce ECG changes indistinguishable from acute OMI. Cardiac cath and/or cardiac MRI may at times be the only ways to arrive at an accurate diagnosis.
= = =
Figure-1: I’ve labeled today’s initial ECG.
= = =
= = =